Peuchant Olivia, Lhomme Edouard, Krêt Marion, Ghezzoul Bellabes, Roussillon Caroline, Bébéar Cécile, Perry Frédéric, de Barbeyrac Bertille
University Bordeaux.
INRA, USC EA 3671, Mycoplasmal and Chlamydial Infections in Humans.
Medicine (Baltimore). 2019 Feb;98(7):e14572. doi: 10.1097/MD.0000000000014572.
Chlamydia trachomatis can lead to a persistent infection in the lower gastrointestinal tract, suggesting a potential role of autoinoculation of cervical chlamydial infection from the rectal site, contributing to repeat infections. Moreover, around 75% of women with urogenital C. trachomatis have concurrent anorectal infection. Current treatment guidelines for urogenital C. trachomatis infection recommend either a single 1 g dose of azithromycin or doxycycline 100 mg twice daily for 7 days. Doxycycline appears to be more effective in treating anorectal infections as suggested in a population of men who have sex with men, but no randomized controlled trial (RCT) had directly compared azithromycin with doxycycline for the treatment of rectal infections. We propose an open-label RCT to compare the microbial cure obtained with a single 1 g dose of azithromycin versus 100 mg of doxycycline twice daily for 7 days, for the treatment of anorectal C. trachomatis infection concurrent to urogenital infection in women.
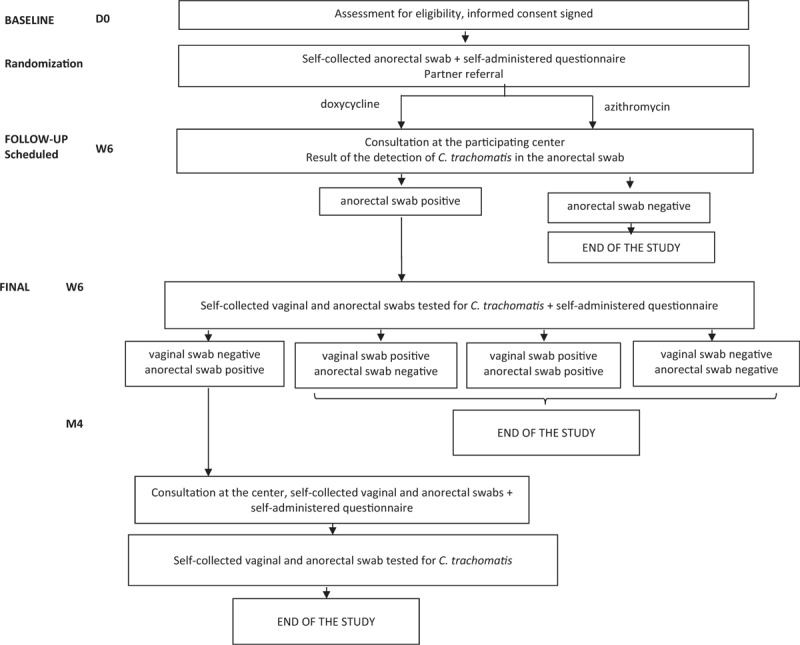
A total of 460 women with C. trachomatis urogenital infection will be enrolled in the study. Women will be asked to provide self-collected anorectal swabs and will be randomized to receive either a 1 g single dose of azithromycin or doxycycline 100 mg twice daily for 7 days. Clinical and biological data will be collected and patients will complete questionnaires about their sexual behavior. The primary outcome is the microbial cure rate, defined as a C. trachomatis negative nucleic acid amplification test (NAAT) result in the anorectal specimens 6 weeks after treatment initiation among women with a C. trachomatis positive urogenital and anorectal NAAT result at the baseline. The secondary outcome is autoinoculation from the rectum to the vagina, which will be evaluated based on the number of women with the same C. trachomatis genotype profile that will be identified in an anorectal-positive specimen obtained 6 weeks after treatment initiation and in a vaginal-positive specimen obtained four months after treatment.
The results of this trial will establish which treatment is more efficacious against anorectal infection and could affect recommendations for the treatment of urogenital C. trachomatis infection, taking into account concurrent anorectal infection.
EudraCT number: 2017-002595-15. CLINICALTRIALS.
NCT03532464. Date of registration: May 31, 2018.
NTC03532464. Secondary ID: CHUBX 2016/26. Date of registration: May 09, 2018.
沙眼衣原体可导致下消化道持续感染,提示存在从直肠部位自体接种宫颈衣原体感染的可能性,这可能导致反复感染。此外,约75%的泌尿生殖系统沙眼衣原体感染女性同时存在肛门直肠感染。目前泌尿生殖系统沙眼衣原体感染的治疗指南推荐单次口服1克阿奇霉素或每日两次口服100毫克多西环素,疗程7天。在男男性行为人群中,多西环素似乎在治疗肛门直肠感染方面更有效,但尚无随机对照试验直接比较阿奇霉素与多西环素治疗直肠感染的效果。我们提议开展一项开放标签随机对照试验,比较单次口服1克阿奇霉素与每日两次口服100毫克多西环素,疗程7天,治疗女性泌尿生殖系统感染并发的肛门直肠沙眼衣原体感染的微生物清除率。
共纳入460例泌尿生殖系统沙眼衣原体感染女性。将要求女性自行采集肛门直肠拭子,并随机分为两组,分别接受单次口服1克阿奇霉素或每日两次口服100毫克多西环素,疗程7天。将收集临床和生物学数据,患者将完成关于其性行为的问卷调查。主要结局是微生物清除率,定义为在基线时泌尿生殖系统和肛门直肠沙眼衣原体核酸扩增试验(NAAT)结果均为阳性的女性中,治疗开始后6周肛门直肠标本沙眼衣原体NAAT结果为阴性。次要结局是从直肠到阴道的自体接种,将根据治疗开始后6周获得的肛门直肠阳性标本和治疗后4个月获得的阴道阳性标本中鉴定出的具有相同沙眼衣原体基因型谱的女性数量进行评估。
本试验结果将确定哪种治疗方法对肛门直肠感染更有效,并可能影响考虑到并发肛门直肠感染时泌尿生殖系统沙眼衣原体感染的治疗建议。
欧洲临床试验数据库编号:2017-002595-15。临床试验注册中心标识符:NCT03532464。注册日期:2018年5月31日。世界卫生组织国际临床试验注册平台:NTC03532464。二级标识符:CHUBX 2016/26。注册日期:2018年5月9日。