Sung Pei-Hsun, Chen Kuan-Hung, Lin Hung-Sheng, Chu Chi-Hsiang, Chiang John Y, Yip Hon-Kan
Division of Cardiology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University, Kaohsiung 83301, Taiwan.
Center for Shockwave Medicine and Tissue Engineering, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung 83301, Taiwan.
J Clin Med. 2019 Feb 5;8(2):190. doi: 10.3390/jcm8020190.
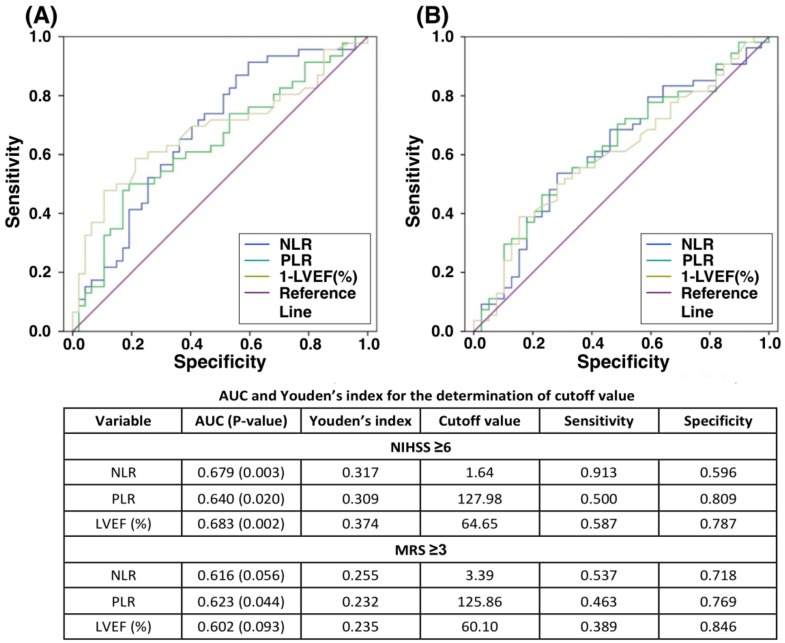
Despite left ventricular (LV) dysfunction increases the risk of incidental acute ischemic stroke (AIS), the association between LV function and severity of neurological deficits after AIS remains unclear. Between November 2015 and October 1017, a total of 99 AIS patients were prospectively enrolled and categorized into two groups based on National Institute of Health Stroke Scale (NIHSS). The AIS patients with NIHSS <6 were allocated into Group 1 ( = 50) and those with NIHSS ≥6 were into Group 2 ( = 49). Echocardiography was performed within 5 days after AIS to assess chamber size, left ventricular ejection fraction (LVEF) and valvular regurgitation. Besides, two inflammatory biomarkers, neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), were evaluated on admission. The results showed Group 2 had significantly higher value of NLR and PLR (all -values < 0.01) but lower LVEF ( = 0.001) and frequency of mitral regurgitation ( = 0.021) than Group 1. The NIHSS and modified Rankin scale were significantly negatively correlated with LVEF, whereas both were significantly positively correlated with NLR and PLR (all -values < 0.02). Multivariate analysis showed LVEF <65%, aging and inflammation were significantly associated with NIHSS ≥6 (all -values < 0.01). In conclusion, the AIS patients with NIHSS ≥6 had lower LVEF but more clinically dominant mitral regurgitation and higher NLR and PLR compared to those with NIHSS <6.
尽管左心室(LV)功能障碍会增加偶发性急性缺血性卒中(AIS)的风险,但LV功能与AIS后神经功能缺损严重程度之间的关联仍不明确。在2015年11月至2017年10月期间,前瞻性纳入了99例AIS患者,并根据美国国立卫生研究院卒中量表(NIHSS)将其分为两组。NIHSS评分<6的AIS患者被分配到第1组(n = 50),NIHSS评分≥6的患者被分到第2组(n = 49)。在AIS发生后5天内进行超声心动图检查,以评估心室大小、左心室射血分数(LVEF)和瓣膜反流情况。此外,入院时评估了两种炎症生物标志物,即中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)。结果显示,与第1组相比,第2组的NLR和PLR值显著更高(所有P值<0.01),但LVEF更低(P = 0.001),二尖瓣反流频率更低(P = 0.021)。NIHSS评分和改良Rankin量表与LVEF显著负相关,而两者均与NLR和PLR显著正相关(所有P值<0.02)。多变量分析显示,LVEF<65%、年龄增长和炎症与NIHSS评分≥6显著相关(所有P值<0.01)。总之,与NIHSS评分<6的AIS患者相比,NIHSS评分≥6的AIS患者LVEF更低,但二尖瓣反流在临床上更占主导地位,且NLR和PLR更高。