Fang Yen-Nan, Tong Meng-Shen, Sung Pei-Hsun, Chen Yung-Lung, Chen Chih-Hung, Tsai Nei-Wen, Huang Chih-Jen, Chang Ya-Ting, Chen Shu-Fang, Chang Wen-Neng, Lu Cheng-Hsien, Yip Hon-Kan
Division of Cardiology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Division of General Medicine, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Biomed J. 2017 Jun;40(3):154-162. doi: 10.1016/j.bj.2017.03.002. Epub 2017 May 30.
We aimed to determine whether higher neutrophil counts (NC) and neutrophil-to-lymphocyte ratio (NLR) were independently predictive of worse in-hospital outcome in patients after acute ischemic stroke (IS).
A retrospective observational study with prospective manner of IS registration. Between April 2012 and August 2014, a total number of 1731 patients with post-IS were consecutively enrolled in the study. Blood samples were drawn upon admission. Primary endpoint was in-hospital mortality. Secondary endpoint was severe stroke (≥16 NIHSS).
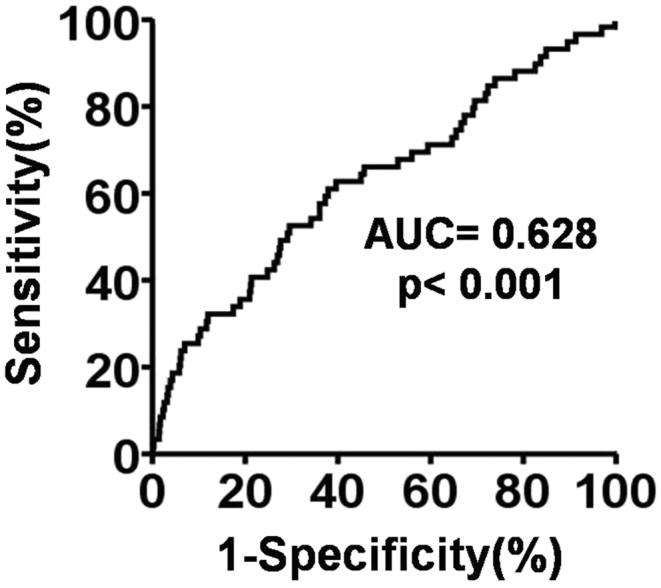
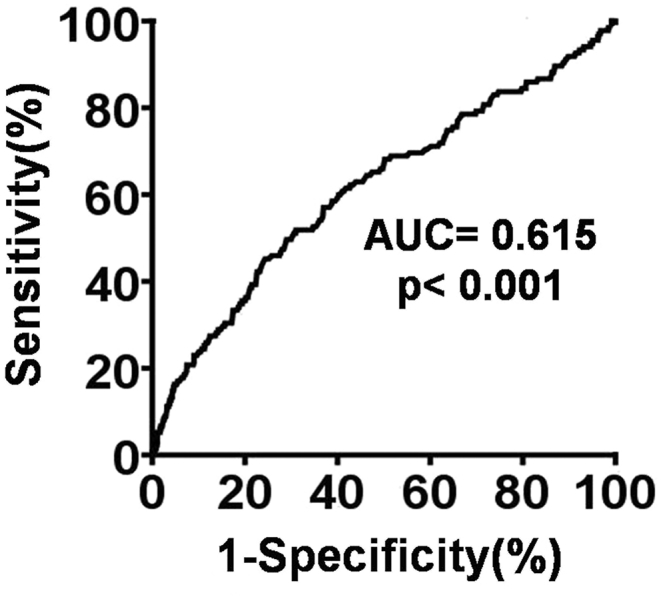
The NC progressively increased from mild (NIHSS ≤ 5) to moderate (NIHSS ≥ 6 < 16) and severe (NIHSS ≥ 16) stroke (p = 0.006). NLR was independently associated with in-hospital mortality (p = 0.002). Multiple stepwise linear regression analysis showed that NC (p = 0.001) and NLR (p = 0.002) were independently predictive of higher NIHSS. Multiple stepwise logistic regression analysis showed that NC was independently associated with severe stroke (p < 0.0001). The best discriminating factor for in-hospital mortality with respect to NLR was ≥3.20 (sensitivity 62.7%, specificity 60.3%, likelihood ratio: 12.2). Patients with NLR ≥3.20 had a 2.55-fold increased risk for in-hospital mortality (OR = 1.49-4.37) compared to patients with NLR <3.20. The best discriminating factor for severe stroke (≥16 NIHSS) with respect to NC was ≥74% (sensitivity 47.1%, specificity 74.0%, likelihood ratio: 29.0). Patients with NC >74% had a 2.54-fold increased risk of severe stroke (OR = 1.82-3.54) compared to patients with NC <74%.
NLR was independently associated with in-hospital mortality and higher NC was independently predictive of severe stroke.
我们旨在确定较高的中性粒细胞计数(NC)和中性粒细胞与淋巴细胞比值(NLR)是否能独立预测急性缺血性卒中(IS)患者更差的院内结局。
一项采用前瞻性IS登记方式的回顾性观察研究。2012年4月至2014年8月期间,共有1731例IS后患者连续纳入本研究。入院时采集血样。主要终点是院内死亡率。次要终点是严重卒中(美国国立卫生研究院卒中量表[NIHSS]≥16分)。
NC从轻度(NIHSS≤5分)卒中逐渐升高至中度(NIHSS≥6分且<16分)和重度(NIHSS≥16分)卒中(p = 0.006)。NLR与院内死亡率独立相关(p = 0.002)。多元逐步线性回归分析显示,NC(p = 0.001)和NLR(p = 0.002)可独立预测更高的NIHSS评分。多元逐步逻辑回归分析显示,NC与严重卒中独立相关(p < 0.0001)。NLR预测院内死亡率的最佳区分因素为≥3.20(敏感性62.7%,特异性60.3%,似然比:12.2)。与NLR<3.20的患者相比,NLR≥3.20的患者院内死亡风险增加2.55倍(比值比[OR]=1.49 - 4.37)。NC预测严重卒中(NIHSS≥16分)的最佳区分因素为≥74%(敏感性47.1%,特异性74.0%,似然比:29.0)。与NC<74%的患者相比,NC>74%的患者发生严重卒中的风险增加2.54倍(OR = 1.82 - 3.54)。
NLR与院内死亡率独立相关,较高的NC可独立预测严重卒中。