Department of Biochemistry, Stanford University School of Medicine, Stanford, CA, 94305, USA.
Cardiovascular Institute, Stanford University School of Medicine, Stanford, CA, 94305, USA.
Pflugers Arch. 2019 May;471(5):701-717. doi: 10.1007/s00424-019-02259-2. Epub 2019 Feb 15.
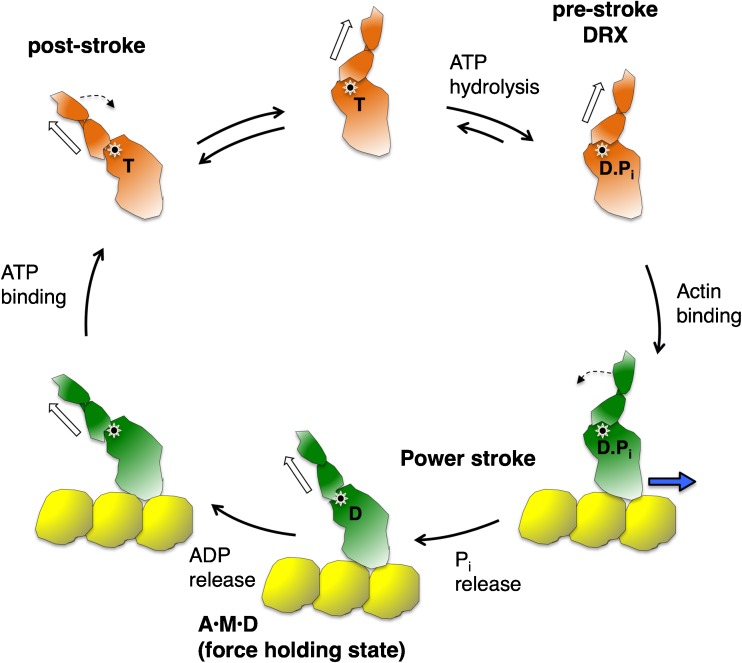
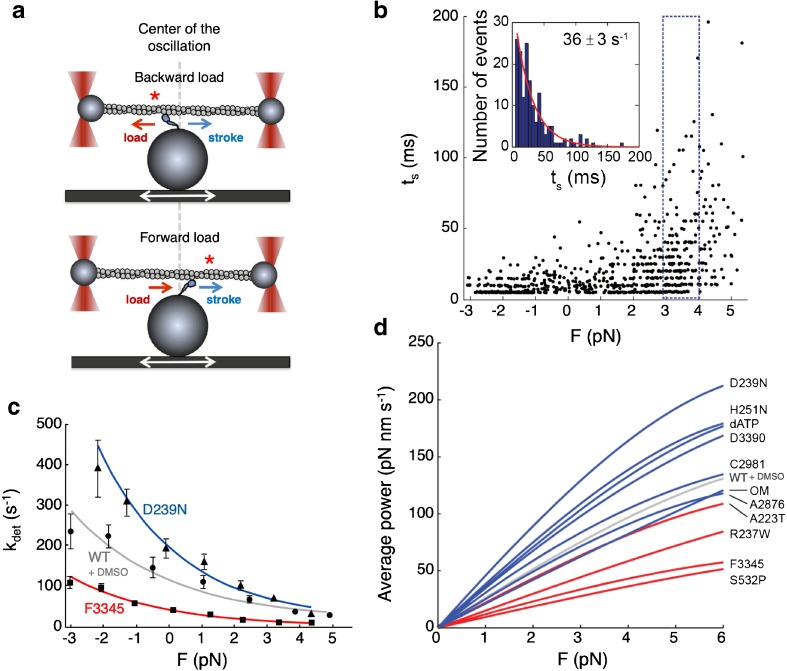
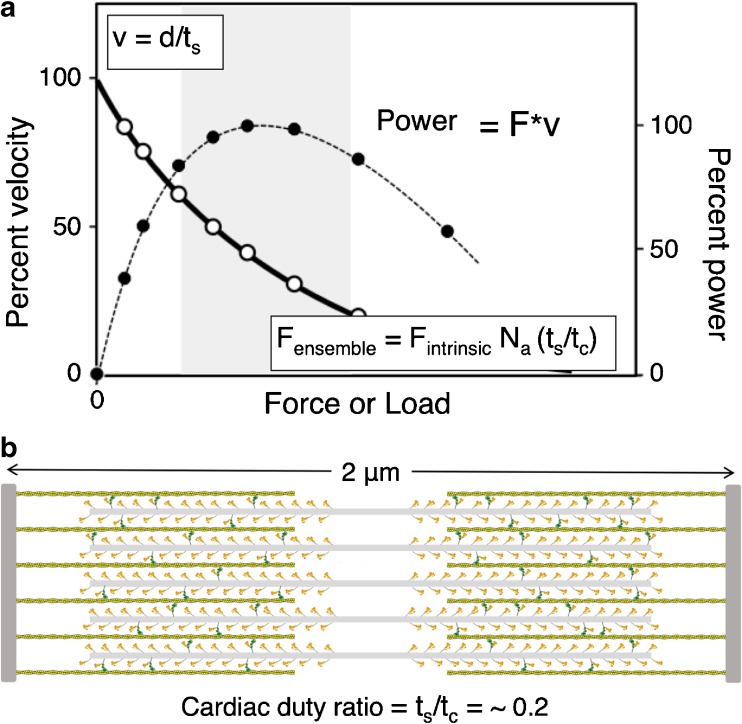
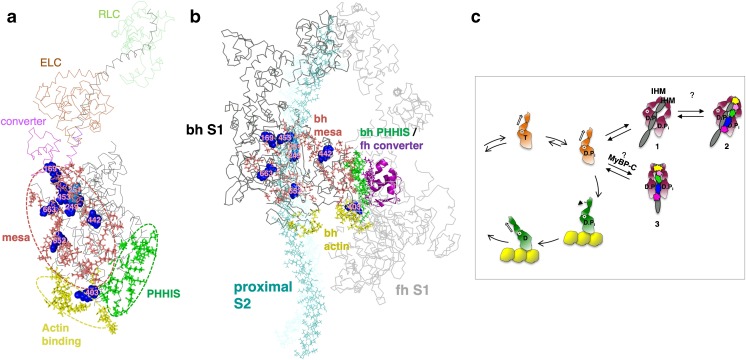
Several lines of evidence suggest that the primary effect of hypertrophic cardiomyopathy mutations in human β-cardiac myosin is hypercontractility of the heart, which leads to subsequent hypertrophy, fibrosis, and myofilament disarray. Here, I describe three perspectives on the molecular basis of this hypercontractility. The first is that hypercontractility results from changes in the fundamental parameters of the actin-activated β-cardiac myosin chemo-mechanical ATPase cycle. The second considers that hypercontractility results from an increase in the number of functionally accessible heads in the sarcomere for interaction with actin. The final and third perspective is that load dependence of contractility is affected by cardiomyopathy mutations and small-molecule effectors in a manner that changes the power output of cardiac contraction. Experimental approaches associated with each perspective are described along with concepts of therapeutic approaches that could prove valuable in treating hypertrophic cardiomyopathy.
有几条证据表明,人类β-心肌球蛋白肥厚型心肌病突变的主要影响是心脏的过度收缩,这导致随后的心肌肥大、纤维化和肌丝排列紊乱。在这里,我描述了这种过度收缩的分子基础的三个观点。第一种观点认为,过度收缩是由于肌球蛋白化学机械 ATP 酶循环的基本参数发生变化所致。第二种观点认为,过度收缩是由于肌节中与肌动蛋白相互作用的功能可及的头部数量增加所致。最后也是第三种观点是,心肌病突变和小分子效应物以改变心脏收缩的功率输出的方式影响收缩的负荷依赖性。本文描述了与每个观点相关的实验方法,以及可能对治疗肥厚型心肌病有价值的治疗方法的概念。