Thrombolysis in Myocardial Infarction (TIMI) Study Group, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USA.
Department of Medicine, Women's College Hospital and the University Health Network, Toronto, Canada.
Eur J Heart Fail. 2019 Apr;21(4):462-470. doi: 10.1002/ejhf.1424. Epub 2019 Feb 18.
Klotho, an essential co-receptor for fibroblast growth factor (FGF)-23, has potentially beneficial inhibitory effects on the renin-angiotensin system. Limited data exist on the prognostic value of Klotho and FGF-23 levels in combination or their ability to predict benefit from angiotensin-converting enzyme (ACE) inhibition.
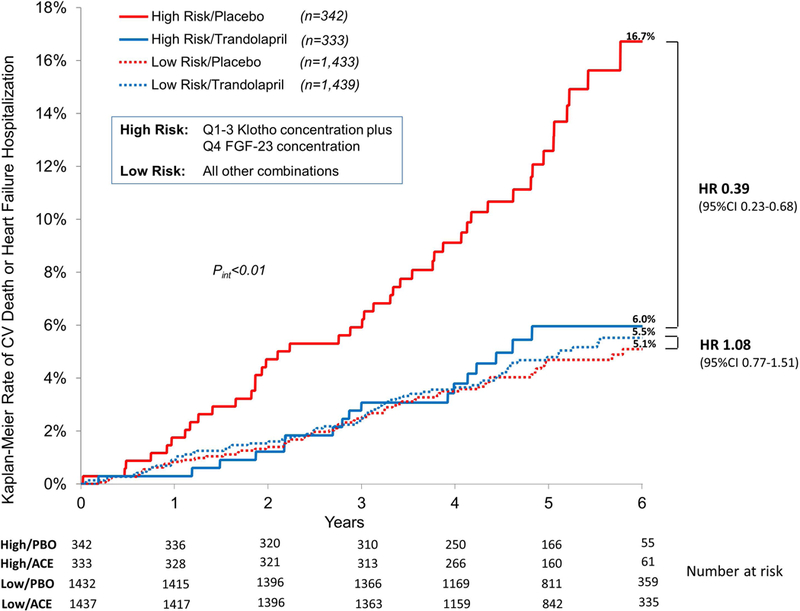
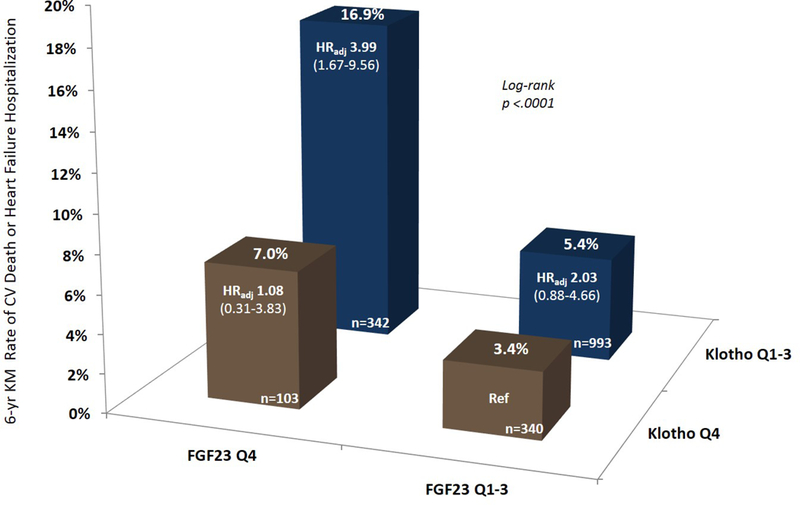
A total of 3555 patients with stable ischaemic heart disease and left ventricular ejection fraction > 40% enrolled in the PEACE trial of trandolapril vs. placebo had Klotho levels drawn at randomization. Patients were characterized by quartiles of Klotho and FGF-23 concentrations. Six-year Kaplan-Meier rates and adjusted risk were calculated in the placebo arm for the composite of cardiovascular (CV) death or hospitalization for heart failure and its components. Low [quartile (Q) 1-3] Klotho concentration was associated with an increased rate of CV death or hospitalization for heart failure as compared with Q4 (8.2% vs. 4.2%; P = 0.03). After multivariable adjustment for clinical variables and renal and CV biomarkers (estimated glomerular filtration rate, cystatin-C, urine albumin-to-creatinine ratio, FGF-23, high-sensitivity troponin T, N-terminal pro-B-type natriuretic peptide, and high-sensitivity C-reactive protein), low Klotho concentration remained strongly associated with increased risk of CV death or hospitalization for heart failure [adjusted hazard ratio (HR) 2.62; 95% confidence interval (CI) 1.35-5.08; P < 0.01]. The combination of low Klotho and high (Q4) FGF-23 concentration identified patients at particularly elevated risk (adjusted HR 3.99; 95% CI 1.67-9.56; P < 0.01). This high-risk combination additionally predicted benefit from trandolapril (HR 0.39; 95% CI 0.23-0.68; P < 0.01).
Low Klotho concentration is associated with an increased risk of CV death or heart failure hospitalization in patients with stable ischaemic heart disease. The combination of low Klotho and high FGF-23 further identifies patients at distinctly elevated risk who derive clinical benefit from the ACE-inhibitor trandolapril.
Klotho 是成纤维细胞生长因子 23(FGF-23)的必需辅助受体,对肾素-血管紧张素系统具有潜在的有益抑制作用。关于 Klotho 和 FGF-23 水平联合或预测血管紧张素转换酶(ACE)抑制剂获益的能力的预后价值的数据有限。
共有 3555 名患有稳定型缺血性心脏病和左心室射血分数>40%的患者参加了曲多普利与安慰剂的 PEACE 试验,在随机分组时抽取了 Klotho 水平。患者按 Klotho 和 FGF-23 浓度四分位数进行特征描述。在安慰剂组中,计算了心血管(CV)死亡或心力衰竭住院的复合终点以及其各组成部分的 6 年 Kaplan-Meier 率和调整风险。与 Q4 相比,低 [四分位数(Q)1-3] Klotho 浓度与 CV 死亡或心力衰竭住院的发生率增加相关(8.2% vs. 4.2%;P=0.03)。在对临床变量以及肾和 CV 生物标志物(估计肾小球滤过率、胱抑素-C、尿白蛋白/肌酐比、FGF-23、高敏肌钙蛋白 T、N 末端 pro-B 型利钠肽和高敏 C 反应蛋白)进行多变量调整后,低 Klotho 浓度仍然与 CV 死亡或心力衰竭住院风险增加密切相关[调整后的危险比(HR)2.62;95%置信区间(CI)1.35-5.08;P<0.01]。低 Klotho 与高(Q4)FGF-23 浓度的组合确定了风险特别升高的患者(调整后的 HR 3.99;95%CI 1.67-9.56;P<0.01)。这种高危组合还预测了曲多普利的获益(HR 0.39;95%CI 0.23-0.68;P<0.01)。
在稳定型缺血性心脏病患者中,低 Klotho 浓度与 CV 死亡或心力衰竭住院风险增加相关。低 Klotho 与高 FGF-23 的组合进一步确定了风险明显升高的患者,他们从 ACE 抑制剂曲多普利中获得临床获益。