Department of Hepato-gastro-enterology, Centre Hospitalier Intercommunal Poissy Saint Germain, Poissy 78300, France.
Department of Statistics, Centre Hospitalier Intercommunal Poissy Saint Germain, Poissy 78300, France.
World J Gastroenterol. 2019 Feb 14;25(6):696-706. doi: 10.3748/wjg.v25.i6.696.
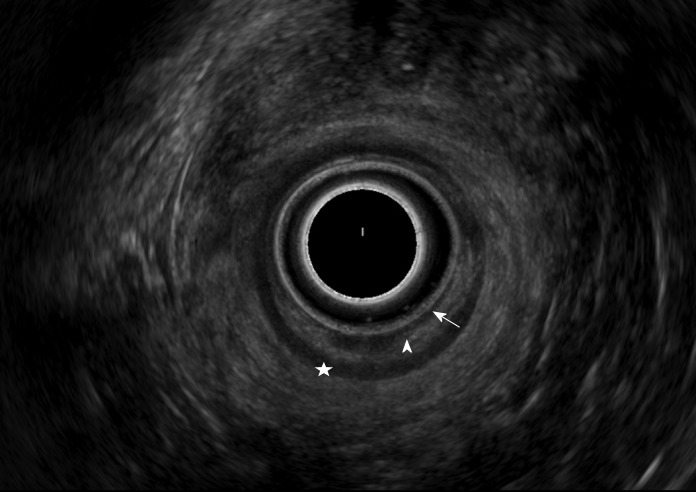
Rectosigmoid endometriosis is an underdiagnosed disease responsible for abdominal pain, transit disorders and rectal bleeding. Two surgical approaches, rectosigmoid bowel resection (segmental or patch) or intramuscular layer dissection (shaving), are available.
To assess whether the lesion features observed preoperative rectosigmoid endoscopic ultrasonography (RS-EUS) might predict the need for bowel resection.
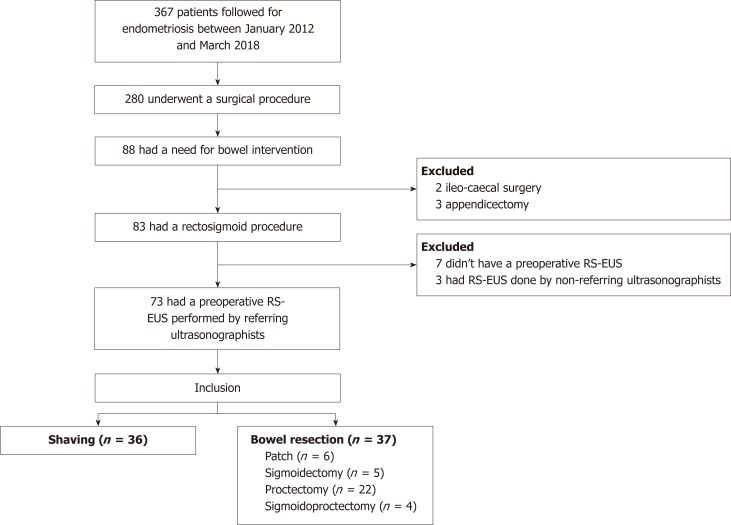
This multicentric retrospective study was conducted on patients with rectosigmoid endometriosis who underwent a curative surgical procedure, evaluated by RS-EUS performed by two trained operators, between January 2012 and March 2018. A univariate statistical analysis was performed on nodules' RS-EUS features (thickness, width, infiltration of the submucosae, presence of a bump into the digestive lumen and presence of multiple rectosigmoid localizations). A multivariate logistic regression was then performed on the significant results.
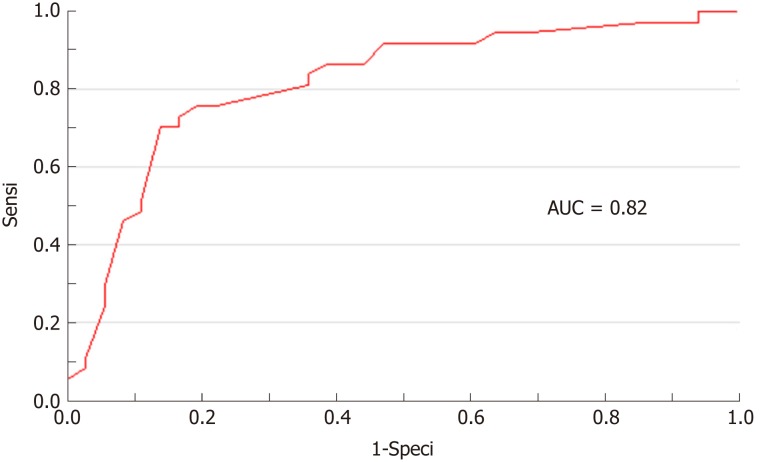
Of the 367 patients, 73 patients with rectosigmoid endometriosis were evaluated by RS-EUS and underwent rectosigmoid surgery. After the univariate analysis was completed, thickness, width and infiltration of the submucosae were identified as potential predictive factors for bowel resection. In a multivariate logistic regression model, only thickness appeared to be a significant [odds ratio (OR) = 1.49, 95% confidence interval (CI): 1.04-2.12, = 0.028] predictive factor for bowel resection. Receiver operating characteristic analysis performed showed that a thickness over 5.20 mm might be used as cut-off with a sensitivity of 76%, a specificity of 81%, and an area under carve = 0.82. The cut-off values for 100% sensitivity and 100% specificity were 0.90 mm and 10.00 mm, respectively. A trend concerning width to predict the need for resection was also observed (OR 1.12, 95%CI: 1.00-1.26, = 0.054).
The presence of a rectosigmoid nodule of endometriosis greater than 5.20 mm thick on RS-EUS might predict the need for bowel resection.
直肠乙状结肠子宫内膜异位症是一种易被漏诊的疾病,其可导致腹痛、排便障碍和直肠出血。目前有两种手术方法,即直肠乙状结肠肠段切除术(节段性或补丁状)或肌层解剖术(刮除术)。
评估术前直肠乙状结肠镜超声(RS-EUS)观察到的病变特征是否可预测肠切除术的需求。
本多中心回顾性研究纳入了 2012 年 1 月至 2018 年 3 月间接受了由两位训练有素的操作者进行的 RS-EUS 评估并接受根治性手术治疗的直肠乙状结肠子宫内膜异位症患者。对结节的 RS-EUS 特征(厚度、宽度、黏膜下浸润、向消化腔隆起和多个直肠乙状结肠定位)进行单变量统计分析。然后对有意义的结果进行多变量逻辑回归分析。
在 367 例患者中,73 例患有直肠乙状结肠子宫内膜异位症并接受 RS-EUS 检查,然后接受了直肠乙状结肠手术。完成单变量分析后,厚度、宽度和黏膜下浸润被确定为肠切除术的潜在预测因素。在多变量逻辑回归模型中,只有厚度是肠切除术的显著预测因子[比值比(OR)=1.49,95%置信区间(CI):1.04-2.12, = 0.028]。受试者工作特征分析显示,厚度超过 5.20mm 可能被用作截断值,其灵敏度为 76%,特异性为 81%,曲线下面积为 0.82。100%灵敏度和 100%特异性的截断值分别为 0.90mm 和 10.00mm。观察到宽度也有预测切除需求的趋势(OR 1.12,95%CI:1.00-1.26, = 0.054)。
RS-EUS 显示直肠乙状结肠结节的厚度大于 5.20mm 可能预测需要肠切除术。