Department of Medicine, University of Missouri, Kansas City, Missouri.
Department of Cardiovascular Research, Saint Luke's Hospital, Kansas City, Missouri.
Cancer Med. 2019 Apr;8(4):1500-1507. doi: 10.1002/cam4.2033. Epub 2019 Feb 21.
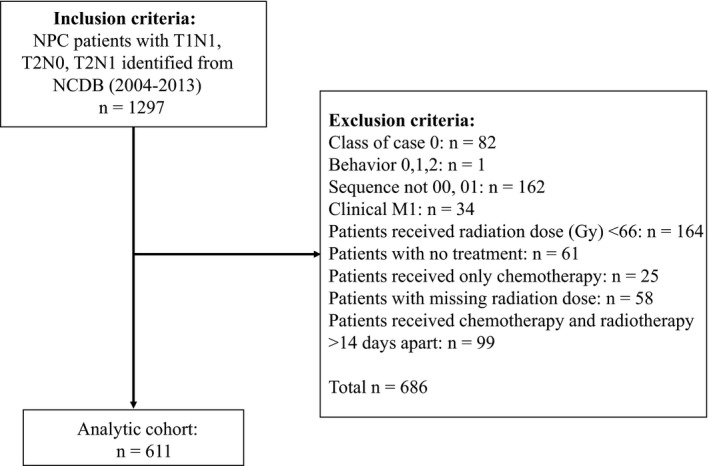
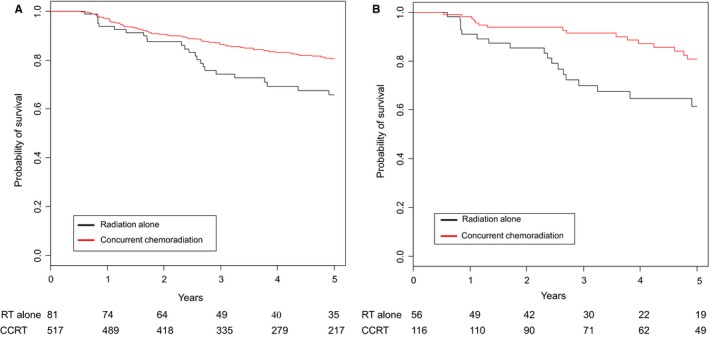
The standard of care treatment for locally advanced nasopharyngeal carcinoma (NPC) includes both chemotherapy and definitive radiation. However, there are limited data on the optimal management of stage II NPC. We performed a retrospective analysis of the National Cancer Database to analyze the treatment patterns and role of chemotherapy in patients with stage II NPC. We identified 611 patients diagnosed with T1-2, N0-1, M0 NPC, from 2004 to 2013. Five-year survival was calculated using Kaplan Meier (KM) analysis. Multivariable analysis and propensity matched analysis were performed to analyze the impact of chemotherapy on overall survival. Of the 611 patients, 527 underwent concurrent chemoradiation (CCRT) and 84 received radiation only. Unadjusted KM analysis showed improved 5-year survival in the CCRT group compared to radiation only (80.5% vs 65.7%; P = 0.0021). Multivariable analysis also showed improved survival with the addition of chemotherapy (Hazard ratio [HR] 0.59; 95 CI 0.39-0.89; P = 0.0124). Propensity matched analysis confirmed a significant clinical benefit from the addition of chemotherapy to radiation. Age ≥ 65 years (HR 2.41; 95% CI 1.71-3.4; P = <0.0001), Charlson-Deyo comorbidity index >1 (HR 2.82; 95% CI 1.49-5.31; P = 0.0014) and positive lymph node status (HR 1.6; 95% CI 1.04-2.46; P = 0.0340) were associated with worse survival. In this retrospective analysis, patients with stage II NPC had improved survival with CCRT compared to definitive radiation only. Elderly patients with comorbidities had worse outcomes.
局部晚期鼻咽癌(NPC)的标准治疗包括化疗和根治性放疗。然而,关于 II 期 NPC 的最佳治疗方法的数据有限。我们对国家癌症数据库进行了回顾性分析,以分析 II 期 NPC 患者的治疗模式和化疗的作用。我们从 2004 年至 2013 年确定了 611 例 T1-2、N0-1、M0 NPC 患者。采用 Kaplan-Meier(KM)分析计算 5 年生存率。进行多变量分析和倾向匹配分析,以分析化疗对总生存率的影响。在 611 例患者中,527 例接受同期放化疗(CCRT),84 例仅接受放疗。未调整的 KM 分析显示,CCRT 组的 5 年生存率高于仅放疗组(80.5%比 65.7%;P=0.0021)。多变量分析还显示,化疗的加入可提高生存率(风险比[HR]0.59;95%置信区间 0.39-0.89;P=0.0124)。倾向匹配分析证实,放疗中加入化疗具有显著的临床获益。年龄≥65 岁(HR 2.41;95%置信区间 1.71-3.4;P<0.0001)、Charlson-Deyo 合并症指数>1(HR 2.82;95%置信区间 1.49-5.31;P=0.0014)和阳性淋巴结状态(HR 1.6;95%置信区间 1.04-2.46;P=0.0340)与生存较差相关。在这项回顾性分析中,与单纯根治性放疗相比,CCRT 治疗的 II 期 NPC 患者的生存得到改善。合并症的老年患者预后较差。