Department of Global Health and Population, Harvard T H Chan School of Public Health, Boston, MA, USA.
Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK; Modelling and Economics Unit, Public Health England, London, UK.
Lancet Glob Health. 2019 Apr;7(4):e472-e481. doi: 10.1016/S2214-109X(18)30537-0. Epub 2019 Feb 21.
In the 21st century, increases in immunisation coverage and decreases in under-5 mortality have substantially reduced the global burden of measles mortality. However, the assessment of measles mortality burden is highly dependent on estimates of case-fatality ratios for measles, which can vary according to geography, health systems infrastructure, prevalence of underlying risk factors, and measles endemicity. With imprecise case-fatality ratios, there is continued uncertainty about the burden of measles mortality and the effect of measles vaccination. In this study, we aimed to update the estimations of case-fatality ratios for measles, to develop a prediction model to estimate case-fatality ratios across heterogeneous groupings, and to project future case-fatality ratios for measles up to 2030.
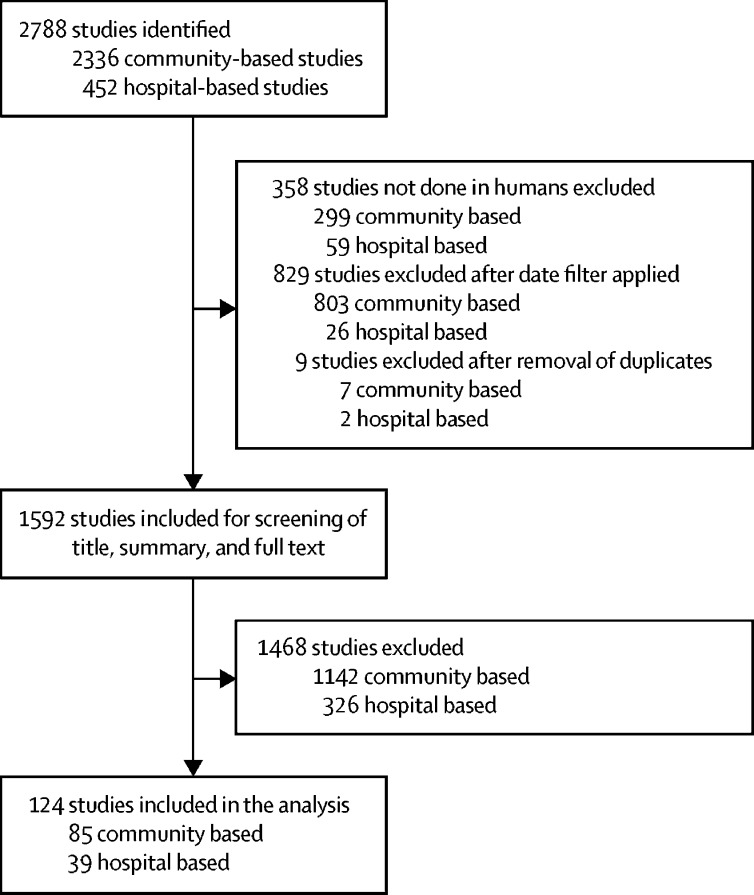
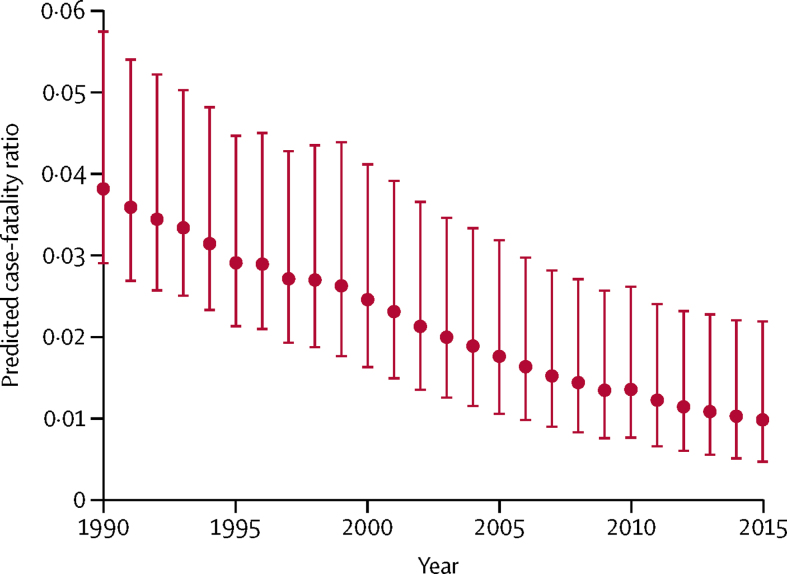
We did a review of the literature to identify studies examining measles cases and deaths in low-income and middle-income countries in all age groups from 1980 to 2016. We extracted data on case-fatality ratios for measles overall and by age, where possible. We developed and examined several types of generalised linear models and determined the best-fit model according to the Akaike information criterion. We then selected a best-fit model to estimate measles case-fatality ratios from 1990 to 2015 and projected future case-fatality ratios for measles up to 2030.
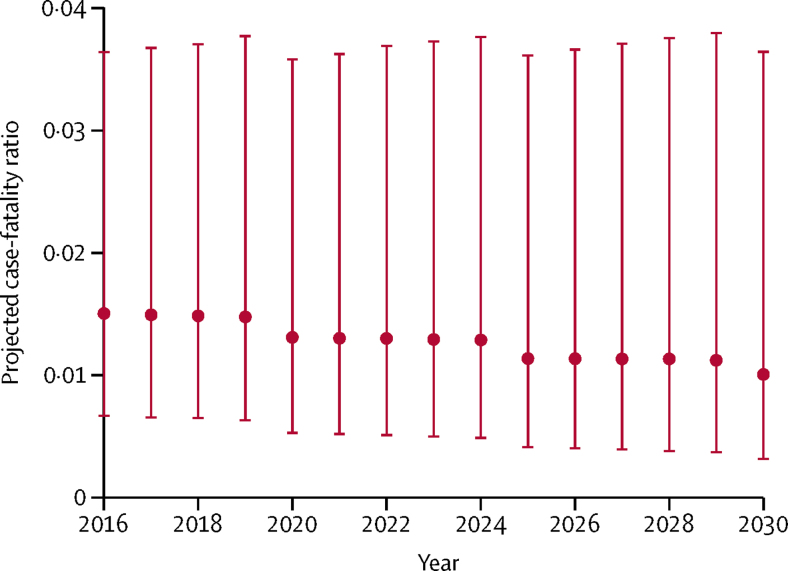
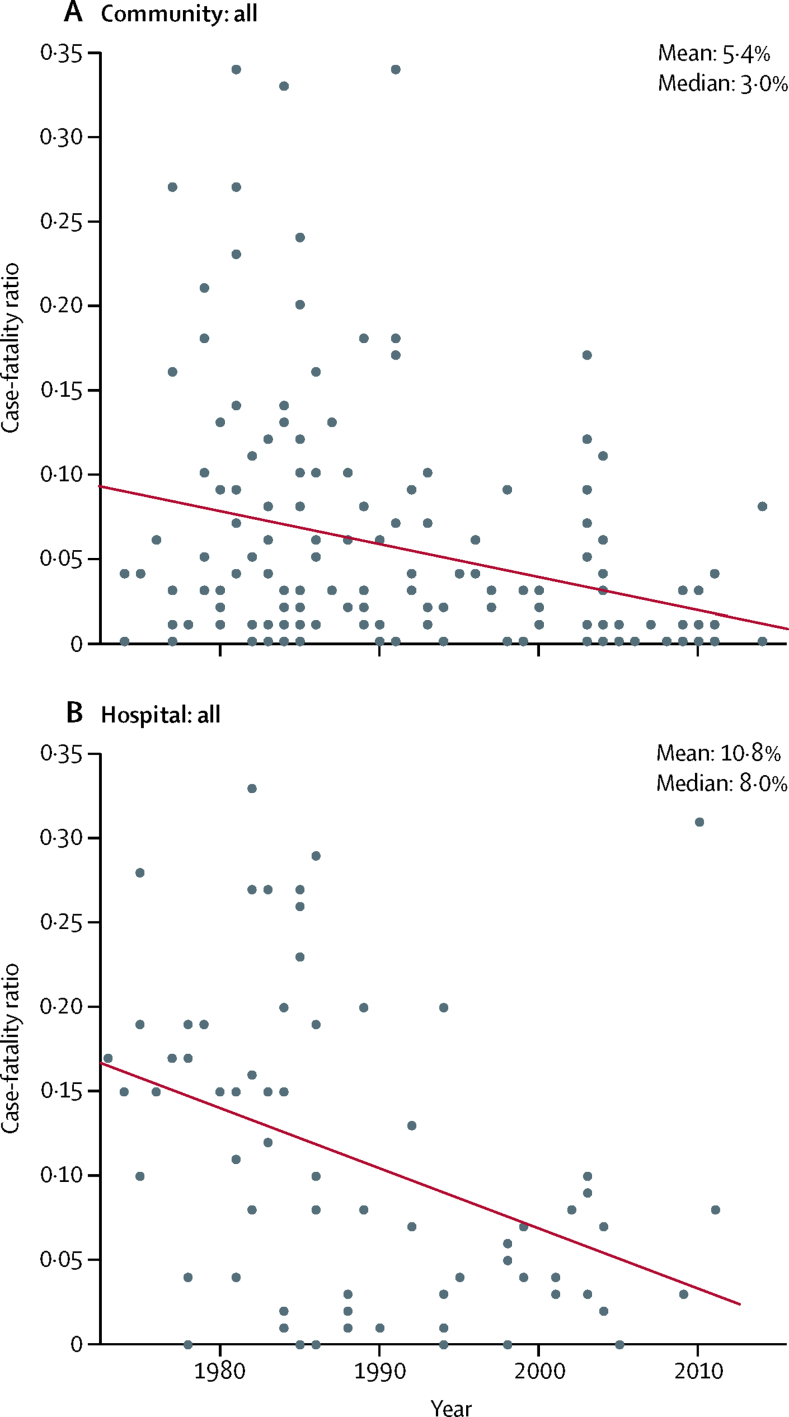
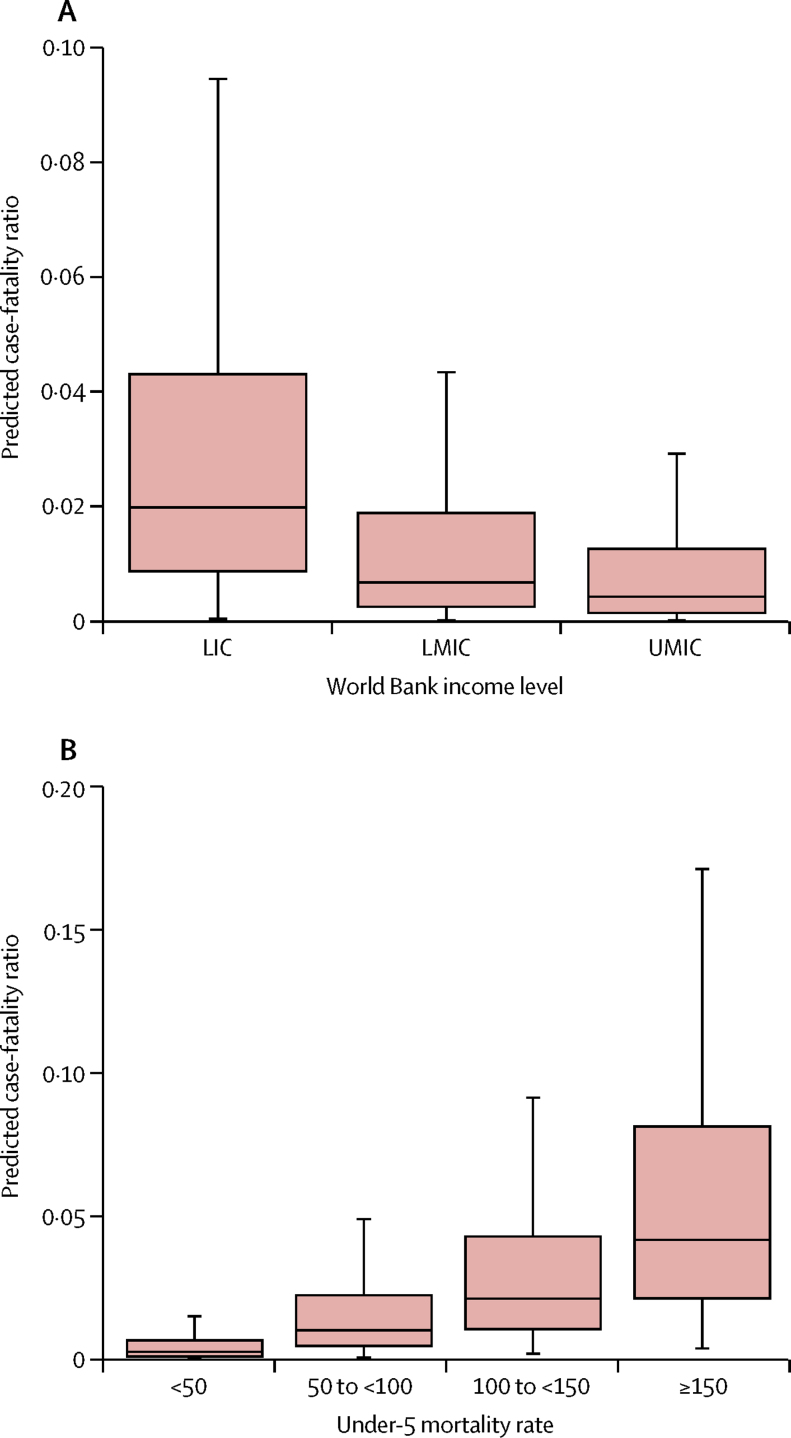
We selected 124 peer-reviewed journal articles published between Jan 1, 1980, and Dec 31, 2016, for inclusion in the final review-85 community-based studies and 39 hospital-based studies. We selected a log-linear prediction model, resulting in a mean case-fatality ratio of 2·2% (95% CI 0·7-4·5) in 1990-2015. In community-based settings, the mean case-fatality ratio was 1·5% (0·5-3·1) compared with 2·9% (0·9-6·0) in hospital-based settings. The mean projected case-fatality ratio in 2016-2030 was 1·3% (0·4-3·7).
Case-fatality ratios for measles have seen substantial declines since the 1990s. Our study provides an updated estimation of case-fatality ratios that could help to refine assessment of the effect on mortality of measles control and elimination programmes.
Bill & Melinda Gates Foundation.
在 21 世纪,免疫覆盖率的提高和 5 岁以下儿童死亡率的降低,大大降低了全球麻疹死亡率。然而,对麻疹死亡率负担的评估高度依赖于对麻疹病死率的估计,而病死率可能因地理位置、卫生系统基础设施、潜在危险因素的流行情况以及麻疹流行情况而有所不同。由于病死率估计不精确,人们对麻疹死亡率的负担以及麻疹疫苗接种的效果仍存在不确定性。在这项研究中,我们旨在更新麻疹病死率的估计值,开发一种预测模型来估计不同分组的病死率,并预测到 2030 年麻疹的病死率。
我们对文献进行了综述,以确定 1980 年至 2016 年期间在所有年龄组中研究低收入和中等收入国家麻疹病例和死亡情况的研究。我们提取了麻疹总体病死率和按年龄分层病死率的数据。我们开发并检查了几种类型的广义线性模型,并根据赤池信息量准则确定了最佳拟合模型。然后,我们选择了一个最佳拟合模型,根据 1990 年至 2015 年的麻疹病死率进行估计,并预测到 2030 年麻疹的病死率。
我们选择了 1980 年 1 月 1 日至 2016 年 12 月 31 日期间发表的 124 篇同行评议的期刊文章进行最终综述,其中包括 85 项社区研究和 39 项医院研究。我们选择了对数线性预测模型,得出 1990 年至 2015 年期间的平均病死率为 2.2%(95%CI 0.7-4.5)。在社区环境中,平均病死率为 1.5%(0.5-3.1),而在医院环境中则为 2.9%(0.9-6.0)。2016 年至 2030 年的平均预测病死率为 1.3%(0.4-3.7)。
自 20 世纪 90 年代以来,麻疹的病死率已大幅下降。我们的研究提供了更新的病死率估计值,有助于更精确地评估麻疹控制和消除规划对死亡率的影响。
比尔及梅琳达·盖茨基金会。