Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia.
Amhara Public Health Institute, Bahir Dar, Ethiopia.
Front Public Health. 2024 May 2;12:1330205. doi: 10.3389/fpubh.2024.1330205. eCollection 2024.
Measles, though usually self-limiting, can have severe consequences influenced by factors such as vaccination and nutrition, notably vitamin A deficiency and malnutrition. Despite progress, contextual changes and implementation issues have hampered efforts, resulting in increased outbreaks and cases of measles. This study seeks to pinpoint outbreak features, risk factors, and strategies for preventing and controlling measles.
A descriptive cross-sectional study and a 1:2 unmatched case-control study design were employed. All 101 suspected measles cases listed on the line-list were included in the descriptive research, with 60 measles patients and 120 controls included in the case-control investigation. Line-list data were cleaned and analyzed using a pivot table in Microsoft Excel 2016. Subsequently, the data were cleaned, entered into Epi Info 7.2, and exported to SPSS 26 for analysis.
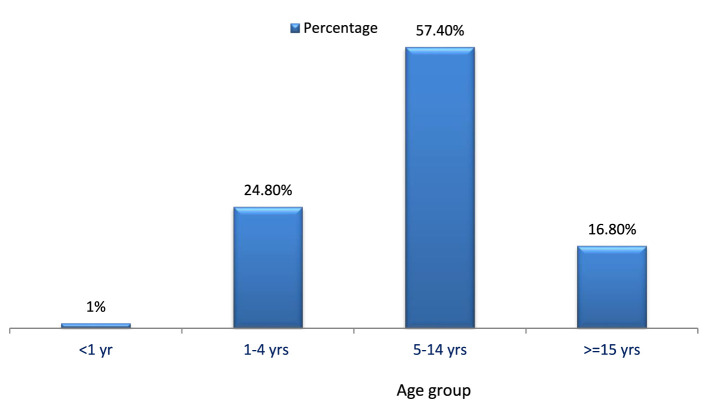
Twenty cases occurred per 10,000 individuals. Men accounted for 67.3% of cases, with ages ranging from 5 months to 45 years and mean and standard deviations of 9.6 and 7.6, respectively. Age group of 5-14 years comprised 57.4% of cases, followed by 1-4 years with 24.8%. Being unvaccinated against measles showed an adjusted odds ratio (AOR) of 12.06 (95% CI: 3.12-46.52). Travel history to regions with active cases had an AOR of 5.73 (95% CI: 1.78-18.38). Contact with a measles patient showed an AOR of 10.3 (95% CI: 3.48-30.5). Understanding the measles transmission mechanism had an AOR of 0.164 (95% CI: 0.049-0.55), and awareness of the disease's preventability had an AOR of 0.233 (95% CI: 0.67-0.811). All factors were independently associated with the illness.
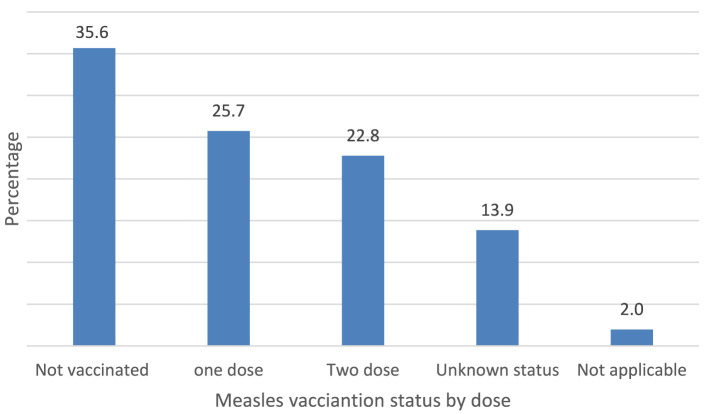
This outbreak affected a broader age range with a high attack rate, mainly in the age group of 5-14-years. Over 35% of cases lacked measles vaccination, indicating low administrative vaccine coverage. Factors contributing to the outbreak include lack of measles vaccination, travel to areas with active disease, contact with cases, and insufficient knowledge of measles transmission and prevention strategies among mothers and caregivers.
麻疹虽然通常是自限性的,但可能会因疫苗接种和营养等因素(如维生素 A 缺乏和营养不良)而产生严重后果。尽管取得了进展,但由于背景变化和实施问题,麻疹的爆发和病例有所增加。本研究旨在确定麻疹爆发的特征、风险因素以及预防和控制麻疹的策略。
采用描述性横断面研究和 1:2 配对病例对照研究设计。描述性研究纳入了名单上列出的 101 例疑似麻疹病例,病例对照研究纳入了 60 例麻疹患者和 120 例对照。使用 Microsoft Excel 2016 中的数据透视表对名单数据进行清洗和分析。随后,将数据清洗后输入 Epi Info 7.2,并导出到 SPSS 26 进行分析。
每 10000 人中有 20 例病例。男性占病例的 67.3%,年龄为 5 个月至 45 岁,平均值和标准差分别为 9.6 和 7.6。5-14 岁年龄组占病例的 57.4%,其次是 1-4 岁年龄组,占 24.8%。麻疹未接种疫苗的调整优势比(AOR)为 12.06(95%可信区间:3.12-46.52)。有麻疹发病地区旅行史的 AOR 为 5.73(95%可信区间:1.78-18.38)。与麻疹患者接触的 AOR 为 10.3(95%可信区间:3.48-30.5)。了解麻疹传播机制的 AOR 为 0.164(95%可信区间:0.049-0.55),了解麻疹可预防的 AOR 为 0.233(95%可信区间:0.67-0.811)。所有因素均与疾病独立相关。
此次麻疹爆发涉及更广泛的年龄范围,发病率较高,主要集中在 5-14 岁年龄组。超过 35%的病例未接种麻疹疫苗,表明行政疫苗覆盖率较低。导致此次爆发的因素包括麻疹疫苗接种不足、前往疾病活跃地区旅行、与病例接触以及母亲和护理人员对麻疹传播和预防策略的了解不足。