Department of Anesthesiology, University Medical Center Groningen, Hanzeplein 1, P.O. Box 30.001, 9700, RB, Groningen, The Netherlands.
Department of Respiratory Medicine, Medizinische Hochschule Hannover, Carl-Neuberg-Straße1, 30625, Hannover, Germany.
BMC Infect Dis. 2019 Feb 26;19(1):195. doi: 10.1186/s12879-019-3820-y.
Patients with pneumonia who are elderly or severely ill are at a particularly high risk of mortality. This post hoc retrospective analysis of data from two Phase III studies evaluated early improvement outcomes in subgroups of high-risk patients with community-acquired pneumonia (CAP) and hospital-acquired pneumonia (HAP, excluding ventilator-associated pneumonia [VAP]).
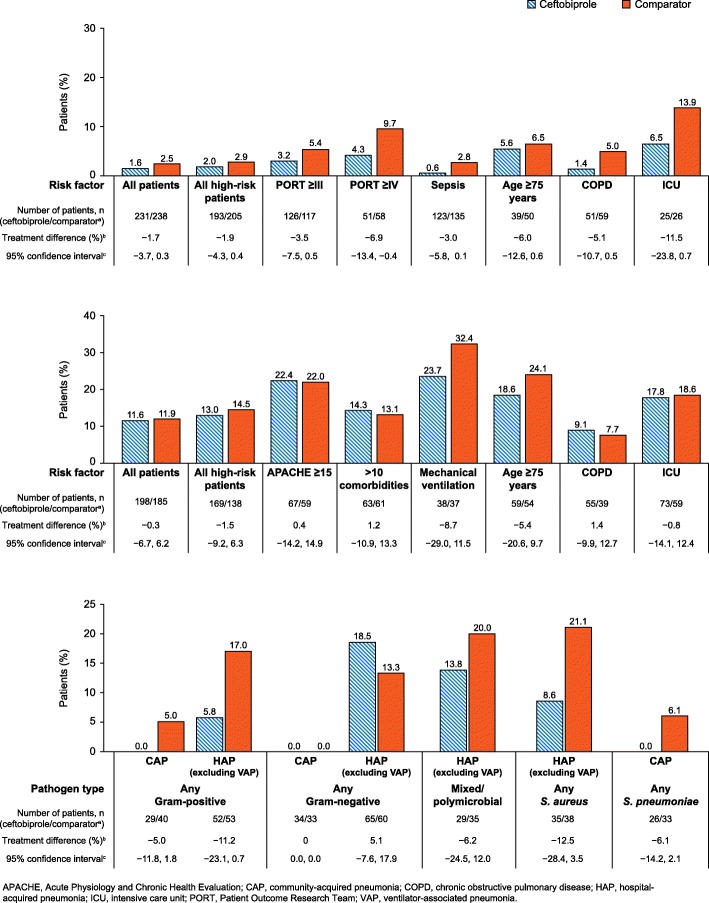
One study included hospitalised CAP patients randomised to ceftobiprole or ceftriaxone ± linezolid treatment. The other study included HAP patients, who were randomised to ceftobiprole or ceftazidime plus linezolid treatment. The primary outcome was rate of early clinical response (Day 3 in CAP and Day 4 in HAP patients). Additional outcome measures included clinical cure at a test-of-cure visit, 30-day all-cause mortality and safety.
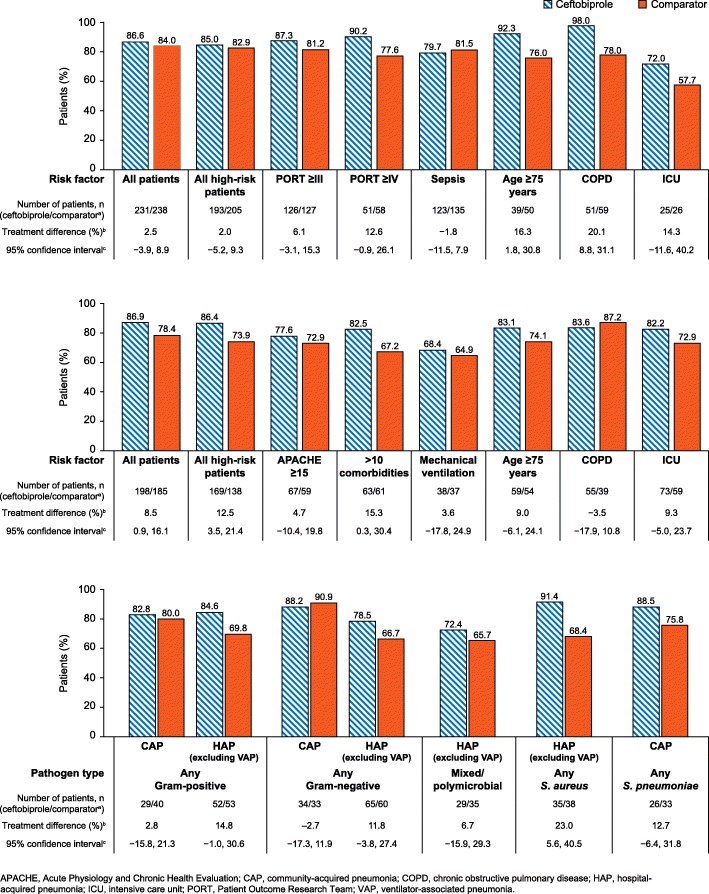
The overall high-risk group comprised 398 CAP patients and 307 HAP patients with risk factors present at baseline. The rate of early response was numerically higher in ceftobiprole-treated patients vs comparator-treated patients in the following high-risk groups: CAP patients aged ≥75 years (16.3% difference, 95% confidence interval [CI]: 1.8, 30.8); CAP patients with COPD (20.1% difference, 95% CI: 8.8, 31.1); all high-risk HAP patients (12.5% difference, 95% CI: 3.5, 21.4); HAP patients with >10 baseline comorbidities (15.3% difference, 95% CI: 0.3, 30.4).
Previous studies show that ceftobiprole is an efficacious therapy for patients with pneumonia who are at high risk of poor outcomes. This post hoc analysis provides preliminary evidence that ceftobiprole treatment may have advantages over other antibiotics in terms of achieving early improvement in high-risk patients with HAP (excluding VAP) and in some subgroups of high-risk CAP patients.
NCT00210964 : registered September 21, 2005; NCT00229008 : registered September 29, 2005; NCT00326287 : registered May 16, 2006.
患有肺炎的老年或重症患者死亡率极高。这是对两项 III 期研究数据的事后回顾性分析,评估了社区获得性肺炎(CAP)和医院获得性肺炎(HAP,不包括呼吸机相关性肺炎[VAP])高危患者亚组的早期改善结局。
一项研究纳入了随机接受头孢比普或头孢曲松±利奈唑胺治疗的住院 CAP 患者。另一项研究纳入了随机接受头孢比普或头孢他啶+利奈唑胺治疗的 HAP 患者。主要结局为早期临床应答率(CAP 患者第 3 天,HAP 患者第 4 天)。其他结局指标包括治愈测试访视时的临床治愈率、30 天全因死亡率和安全性。
总体高危组包括 398 例 CAP 患者和 307 例 HAP 患者,这些患者在基线时存在危险因素。在以下高危亚组中,头孢比普治疗组的早期应答率高于对照组:≥75 岁的 CAP 患者(16.3%差异,95%置信区间[CI]:1.8,30.8);合并 COPD 的 CAP 患者(20.1%差异,95% CI:8.8,31.1);所有高危 HAP 患者(12.5%差异,95% CI:3.5,21.4);存在>10 种基线合并症的 HAP 患者(15.3%差异,95% CI:0.3,30.4)。
既往研究显示,头孢比普对预后不良风险较高的肺炎患者是一种有效的治疗方法。本事后分析提供了初步证据,表明头孢比普治疗可能优于其他抗生素,可改善某些高危 CAP 患者亚组和 HAP(不包括 VAP)高危患者的早期改善。
NCT00210964:2005 年 9 月 21 日注册;NCT00229008:2005 年 9 月 29 日注册;NCT00326287:2006 年 5 月 16 日注册。