Braga Antonio, Mora Paulo, de Melo Andréia Cristina, Nogueira-Rodrigues Angélica, Amim-Junior Joffre, Rezende-Filho Jorge, Seckl Michael J
Postgraduate Program of Medical Sciences, Fluminense Federal University, Niterói 24033-900, Brazil.
Brazilian National Cancer, Hospital do Câncer 2, Rio de Janeiro 20220-410, Brazil.
World J Clin Oncol. 2019 Feb 24;10(2):28-37. doi: 10.5306/wjco.v10.i2.28.
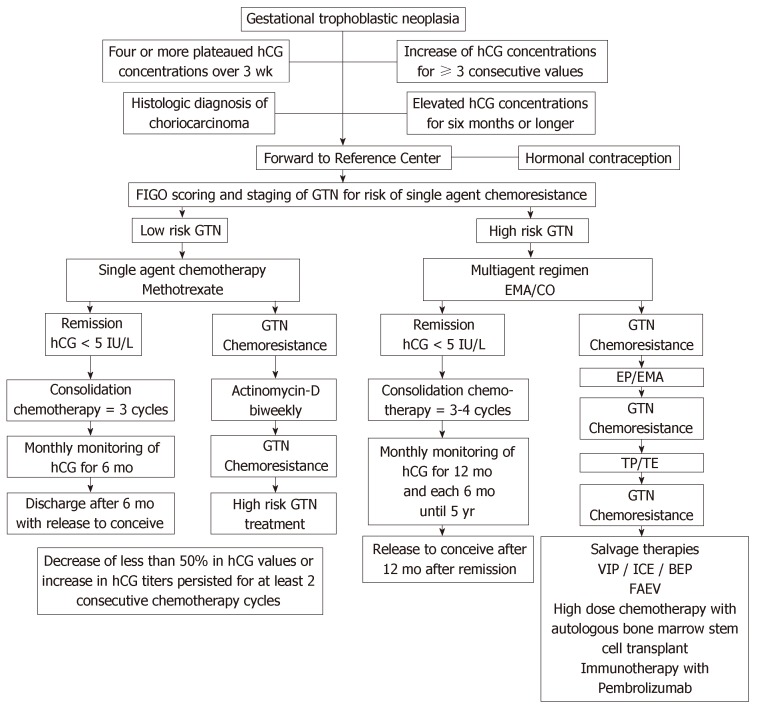
Gestational trophoblastic neoplasia (GTN) is a rare tumor that originates from pregnancy that includes invasive mole, choriocarcinoma (CCA), placental site trophoblastic tumor and epithelioid trophoblastic tumor (PSTT/ETT). GTN presents different degrees of proliferation, invasion and dissemination, but, if treated in reference centers, has high cure rates, even in multi-metastatic cases. The diagnosis of GTN following a hydatidiform molar pregnancy is made according to the International Federation of Gynecology and Obstetrics (FIGO) 2000 criteria: four or more plateaued human chorionic gonadotropin (hCG) concentrations over three weeks; rise in hCG for three consecutive weekly measurements over at least a period of 2 weeks or more; and an elevated but falling hCG concentrations six or more months after molar evacuation. However, the latter reason for treatment is no longer used by many centers. In addition, GTN is diagnosed with a pathological diagnosis of CCA or PSTT/ETT. For staging after a molar pregnancy, FIGO recommends pelvic-transvaginal Doppler ultrasound and chest X-ray. In cases of pulmonary metastases with more than 1 cm, the screening should be complemented with chest computed tomography and brain magnetic resonance image. Single agent chemotherapy, usually Methotrexate (MTX) or Actinomycin-D (Act-D), can cure about 70% of patients with FIGO/World Health Organization (WHO) prognosis risk score ≤ 6 (low risk), reserving multiple agent chemotherapy, such as EMA/CO (Etoposide, MTX, Act-D, Cyclophosphamide and Oncovin) for cases with FIGO/WHO prognosis risk score ≥ 7 (high risk) that is often metastatic. Best overall cure rates for low and high risk disease is close to 100% and > 95%, respectively. The management of PSTT/ETT differs and cure rates tend to be a bit lower. The early diagnosis of this disease and the appropriate treatment avoid maternal death, allow the healing and maintenance of the reproductive potential of these women.
妊娠滋养细胞肿瘤(GTN)是一种起源于妊娠的罕见肿瘤,包括侵袭性葡萄胎、绒毛膜癌(CCA)、胎盘部位滋养细胞肿瘤和上皮样滋养细胞肿瘤(PSTT/ETT)。GTN呈现出不同程度的增殖、侵袭和扩散,但如果在参考中心进行治疗,即使是多转移病例,治愈率也很高。葡萄胎妊娠后GTN的诊断依据国际妇产科联合会(FIGO)2000标准:在三周内人绒毛膜促性腺激素(hCG)浓度出现四次或更多次平台期;至少连续两周每周测量hCG持续上升;葡萄胎排空后六个月或更长时间hCG浓度升高但呈下降趋势。然而,后一种治疗依据目前许多中心已不再使用。此外,GTN通过CCA或PSTT/ETT的病理诊断来确诊。对于葡萄胎妊娠后的分期,FIGO建议采用经阴道盆腔多普勒超声和胸部X线检查。对于肺部转移灶直径大于1 cm的病例,筛查应辅以胸部计算机断层扫描和脑部磁共振成像。单药化疗,通常是甲氨蝶呤(MTX)或放线菌素-D(Act-D),可治愈约70%的FIGO/世界卫生组织(WHO)预后风险评分≤6(低风险)的患者,对于FIGO/WHO预后风险评分≥7(高风险)且常发生转移的病例,则采用多药联合化疗,如EMA/CO(依托泊苷、MTX、Act-D、环磷酰胺和长春新碱)。低风险和高风险疾病的最佳总体治愈率分别接近100%和>95%。PSTT/ETT的治疗方法不同,治愈率往往略低。该疾病的早期诊断和适当治疗可避免孕产妇死亡,使这些女性的生殖潜能得以恢复和维持。