Department of Intensive Care and Anaesthesia, Saint James's Hospital, Dublin, Ireland.
School of Medicine, Trinity College Dublin, College Green, Dublin, Ireland.
PLoS One. 2019 Feb 28;14(2):e0212438. doi: 10.1371/journal.pone.0212438. eCollection 2019.
Poor quality communication between hospital doctors and GPs at the time of hospital discharge is associated with adverse patient outcomes. This may be more marked after an episode of critical illness, the complications of which can persist long after hospital discharge.
Parallel mixed methods observational study in an Irish setting, with equal emphasis on quantitative and qualitative data. Descriptive analysis was performed on quantitative data derived from GP and ICU consultant questionnaires. Qualitative data came from semi-structured interviews with GPs and consultants, and were analysed using directed content analysis. Mixing of data occurred at the stage of interpretation.
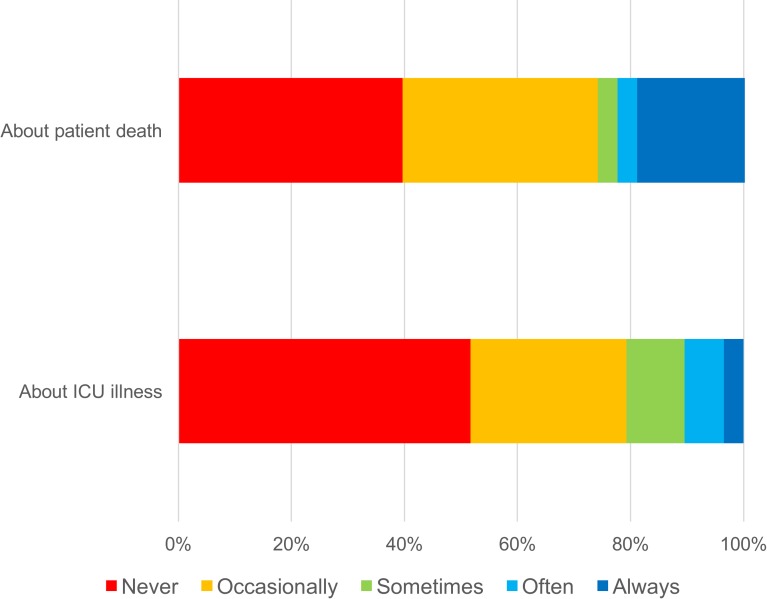
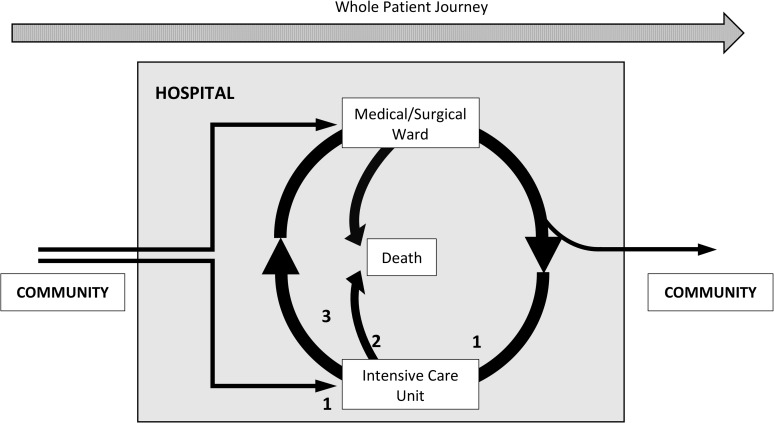
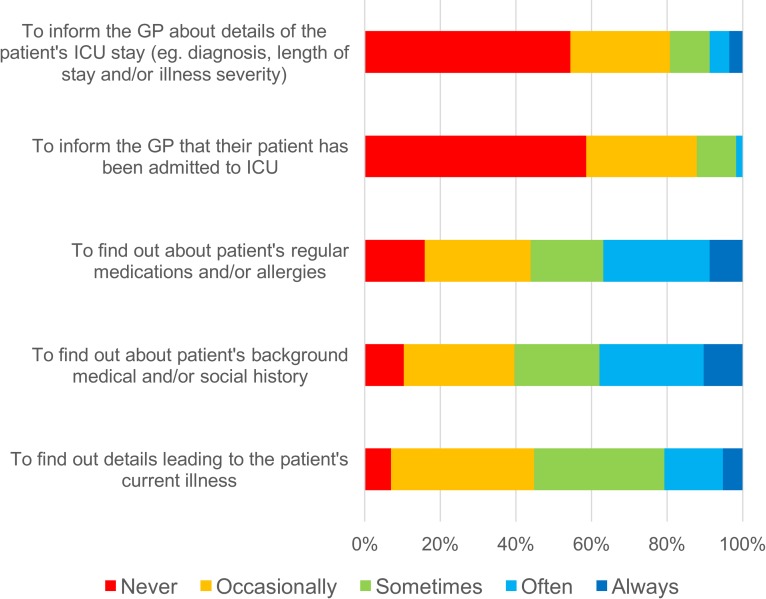
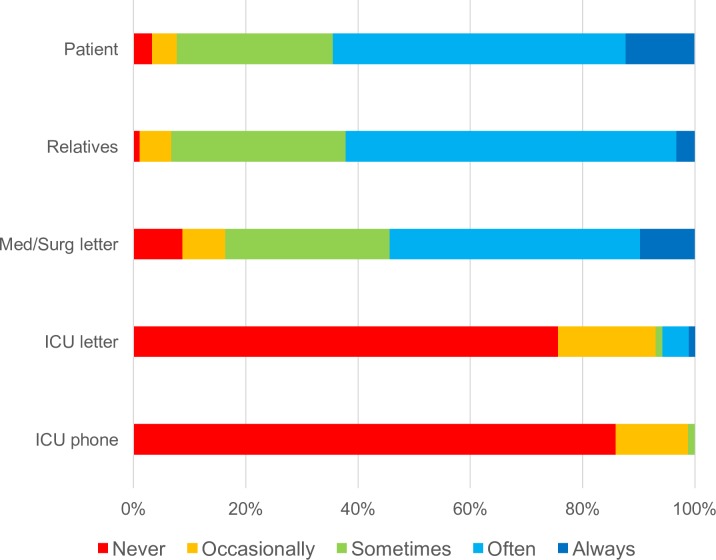
GPs rarely received information about an episode of critical illness directly from ICU staff, with most coming from patients and relatives. Information received from hospital sources was frequently brief and incomplete. Common communication barriers reported by consultants were insufficient time, low perceived importance and difficulty establishing GP contact. When provided information, GPs seldom actioned specific interventions, citing insufficient guidance in hospital correspondence and poor knowledge about critical illness complications and their management. A majority of all respondents thought that improved information sharing would benefit patients. Cultural influences on practice were identified in qualitative data. A priori qualitative themes were: (1) perceived benefits of information sharing, (2) factors influencing current practice and (3) strategies for optimal information sharing. Emergent themes were: (4) the central role of the GP in patient care, (5) the concept of the "whole patient journey" and (6) a culture of expectation around a GP's knowledge of hospital care.
Practical and cultural factors contribute to suboptimal information sharing between ICU and primary care doctors around an episode of critical illness in ICU. We propose a three-milestone strategy to improve the flow and utilisation of information when patients are admitted, discharged or die within the ICU.
医院医生和全科医生在出院时沟通质量差与患者预后不良有关。在经历危重疾病后,这种情况可能更为明显,因为疾病的并发症在出院后很长时间内仍然存在。
在爱尔兰进行的一项平行混合方法观察性研究,定量和定性数据同等重视。对来自全科医生和 ICU 顾问问卷的定量数据进行描述性分析。定性数据来自全科医生和顾问的半结构化访谈,使用定向内容分析进行分析。数据在解释阶段进行混合。
全科医生很少直接从 ICU 工作人员那里收到有关危重病发作的信息,大多数信息来自患者和家属。从医院来源收到的信息通常简短且不完整。顾问报告的常见沟通障碍包括时间不足、感知重要性低和难以与全科医生联系。当提供信息时,全科医生很少采取具体干预措施,理由是医院通信中缺乏指导和对危重病并发症及其管理的知识有限。大多数受访者认为,改善信息共享将使患者受益。定性数据中确定了文化对实践的影响。预先确定的定性主题是:(1) 信息共享的感知益处,(2) 当前实践的影响因素,(3) 优化信息共享的策略。出现的主题是:(4) 全科医生在患者护理中的核心作用,(5) “患者整个就医过程”的概念,以及 (6) 全科医生对医院护理知识的期望文化。
在 ICU 中,与危重病相关的 ICU 和初级保健医生之间的信息共享存在实际和文化因素的制约。我们提出了一个三步策略,以改善患者在 ICU 中入院、出院或死亡时的信息流动和利用。