Department of Anesthesiology, The Jikei University School of Medicine, Tokyo 105-8491, Japan
Center for Critical Care Nephrology, Department of Critical Care Medicine, University of Pittsburgh, Pittsburgh, PA, USA.
BMJ. 2019 Feb 28;364:l430. doi: 10.1136/bmj.l430.
To determine survival associated with advanced airway management (AAM) compared with no AAM for adults with out-of-hospital cardiac arrest.
Cohort study between January 2014 and December 2016.
Nationwide, population based registry in Japan (All-Japan Utstein Registry).
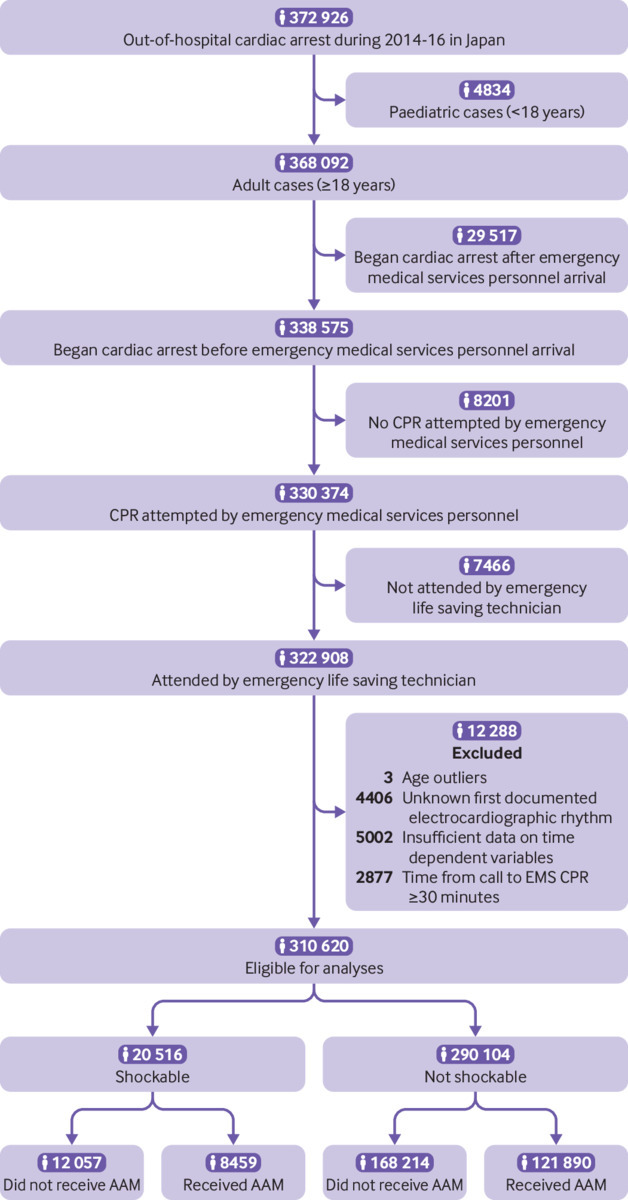
Consecutive adult patients with out-of-hospital cardiac arrest, separated into two sub-cohorts by their first documented electrocardiographic rhythm: shockable (ventricular fibrillation or pulseless ventricular tachycardia) and non-shockable (pulseless electrical activity or asystole). Patients who received AAM during cardiopulmonary resuscitation were sequentially matched with patients at risk of AAM within the same minute on the basis of time dependent propensity scores.
Survival at one month or at hospital discharge within one month.
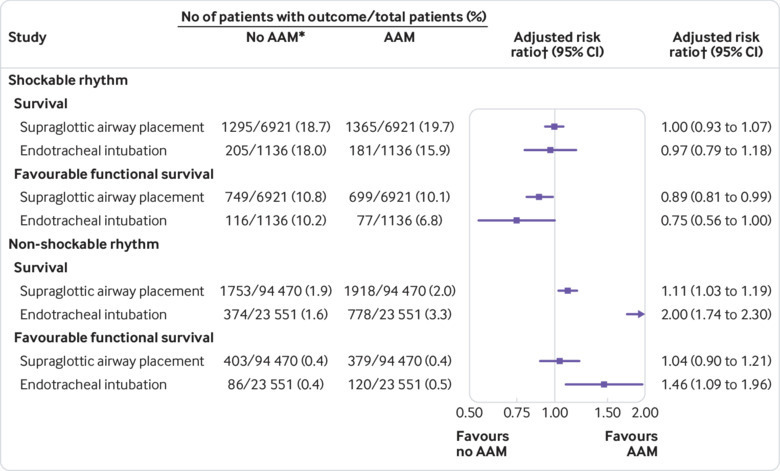
Of the 310 620 patients eligible, 8459 (41.2%) of 20 516 in the shockable cohort and 121 890 (42.0%) of 290 104 in the non-shockable cohort received AAM during cardiopulmonary resuscitation. After time dependent propensity score sequential matching, 16 114 patients in the shockable cohort and 236 042 in the non-shockable cohort were matched at the same minute. In the shockable cohort, survival did not differ between patients with AAM and those with no AAM: 1546/8057 (19.2%) versus 1500/8057 (18.6%) (adjusted risk ratio 1.00, 95% confidence interval 0.93 to 1.07). In the non-shockable cohort, patients with AAM had better survival than those with no AAM: 2696/118 021 (2.3%) versus 2127/118 021 (1.8%) (adjusted risk ratio 1.27, 1.20 to 1.35).
In the time dependent propensity score sequential matching for out-of-hospital cardiac arrest in adults, AAM was not associated with survival among patients with shockable rhythm, whereas AAM was associated with better survival among patients with non-shockable rhythm.
确定与成人院外心脏骤停时的高级气道管理(AAM)相比,无 AAM 相关的生存情况。
2014 年 1 月至 2016 年 12 月进行的队列研究。
日本全国性、基于人群的注册中心(全日本 Utstein 注册中心)。
连续纳入院外心脏骤停的成年患者,根据首次记录的心电图节律分为两个亚组:可电击(心室颤动或无脉性室性心动过速)和不可电击(无脉性电活动或心搏停止)。在心肺复苏期间接受 AAM 的患者根据时间依赖性倾向评分,与同一分钟内有 AAM 风险的患者进行连续匹配。
一个月时或一个月内出院时的生存情况。
在 310620 名符合条件的患者中,20516 名可电击组中的 8459 名(41.2%)和 290104 名不可电击组中的 121890 名(42.0%)在心肺复苏期间接受了 AAM。在时间依赖性倾向评分连续匹配后,可电击组中有 16114 名患者和不可电击组中有 236042 名患者在同一分钟内进行了匹配。在可电击组中,接受 AAM 的患者与未接受 AAM 的患者之间的生存率无差异:8057 名患者中有 1546 名(19.2%)与 8057 名患者中有 1500 名(18.6%)(调整风险比 1.00,95%置信区间 0.93 至 1.07)。在不可电击组中,接受 AAM 的患者比未接受 AAM 的患者生存率更高:118021 名患者中有 2696 名(2.3%)与 118021 名患者中有 2127 名(1.8%)(调整风险比 1.27,1.20 至 1.35)。
在成人院外心脏骤停的时间依赖性倾向评分连续匹配中,AAM 与可电击节律患者的生存率无关,而与不可电击节律患者的生存率相关。