Division of Renal Medicine, Brigham and Women's Hospital, Harvard Medical School, One Brigham Circle, Boston, MA, 02115, USA.
Partners Healthcare, Partners eCare, Boston, MA, USA.
BMC Nephrol. 2019 Mar 1;20(1):72. doi: 10.1186/s12882-019-1260-y.
Electronic health record (EHR) based chronic kidney disease (CKD) registries are central to population health strategies to improve CKD care. In 2015, Partners Healthcare System (PHS), encompassing multiple academic and community hospitals and outpatient care facilities in Massachusetts, developed an EHR-based CKD registry to identify opportunities for quality improvement, defined as improvement on both process measures and outcomes measures associated with clinical care.
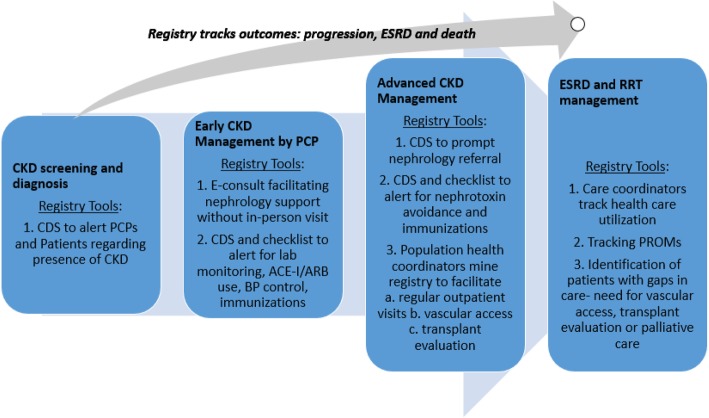
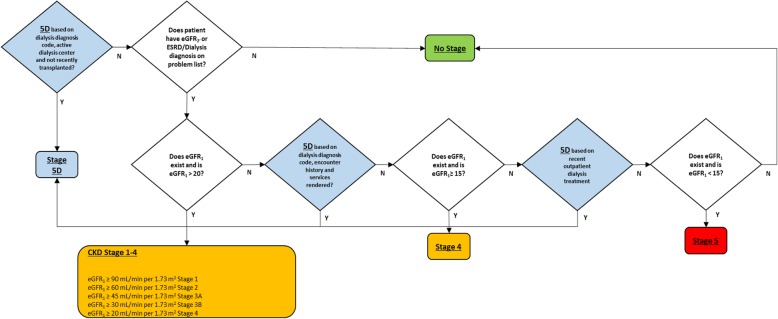
Patients are included in the registry based on the following criteria: 1) two estimated glomerular filtration rate (eGFR) results < 60 ml/min/1.73m separated by 90 days, including the most recent eGFR being < 60 ml/min/1.73m; or 2) the most recent two urine protein values > 300 mg protein/g creatinine on either urine total protein/creatinine ratio or urine albumin/creatinine ratio; or 3) an EHR problem list diagnosis of end stage renal disease (ESRD). The registry categorizes patients by CKD stage and includes rates of annual testing for eGFR and proteinuria, blood pressure control, use of angiotensin converting enzyme inhibitors (ACE-Is) or angiotensin receptor blockers (ARBs), nephrotoxic medication use, hepatitis B virus (HBV) immunization, vascular access placement, transplant status, CKD progression risk; number of outpatient nephrology visits, and hospitalizations.
The CKD registry includes 60,503 patients and has revealed several opportunities for care improvement including 1) annual proteinuria testing performed for 17% (stage 3) and 31% (stage 4) of patients; 2) ACE-I/ARB used in 41% (stage 3) and 46% (stage 4) of patients; 3) nephrotoxic medications used among 23% of stage 4 patients; and 4) 89% of stage 4 patients lack HBV immunity. For advanced CKD patients there are opportunities to improve vascular access placement, transplant referrals and outpatient nephrology contact.
A CKD registry can identify modifiable care gaps across the spectrum of CKD care and enable population health strategy implementation. No linkage to Social Security Death Master File or US Renal Data System (USRDS) databases limits our ability to track mortality and progression to ESRD.
电子健康记录(EHR)为基础的慢性肾脏病(CKD)登记系统是改善 CKD 护理的人群健康策略的核心。2015 年,包括马萨诸塞州多家学术和社区医院以及门诊护理设施在内的合作伙伴医疗系统(PHS)开发了一个基于 EHR 的 CKD 登记系统,以确定改善质量的机会,这一定义为与临床护理相关的流程措施和结果措施的改善。
患者符合以下标准之一即被纳入登记系统:1)两次肾小球滤过率(eGFR)结果<60ml/min/1.73m,间隔 90 天,包括最近一次 eGFR<60ml/min/1.73m;或 2)最近两次尿蛋白值>300mg 蛋白/g 肌酐,分别用尿总蛋白/肌酐比值或尿白蛋白/肌酐比值表示;或 3)EHR 问题列表诊断为终末期肾病(ESRD)。该登记系统根据 CKD 分期对患者进行分类,包括 eGFR 和蛋白尿的年度检测率、血压控制率、血管紧张素转换酶抑制剂(ACE-Is)或血管紧张素受体阻滞剂(ARBs)的使用率、肾毒性药物使用率、乙型肝炎病毒(HBV)免疫接种率、血管通路的建立情况、移植状态、CKD 进展风险、门诊肾科就诊次数和住院次数。
CKD 登记系统包含 60503 名患者,揭示了一些改进护理的机会,包括 1)31%(第 4 期)和 17%(第 3 期)的患者进行年度蛋白尿检测;2)46%(第 4 期)和 41%(第 3 期)的患者使用 ACE-I/ARB;3)23%的第 4 期患者使用肾毒性药物;4)89%的第 4 期患者缺乏 HBV 免疫力。对于晚期 CKD 患者,有机会改善血管通路的建立、移植转诊和门诊肾科联系。
CKD 登记系统可以识别整个 CKD 护理范围内可改变的护理差距,并使人群健康策略的实施成为可能。与社会保障死亡主文件或美国肾脏数据系统(USRDS)数据库没有链接限制了我们跟踪死亡率和进展为 ESRD 的能力。