Department of Physiology, Faculty of Medicine and Nursing, University of the Basque Country (UPV/EHU), Leioa, Bizkaia, Spain.
CNRS, RMSB, UMR 5536, Bordeaux, France.
J Cachexia Sarcopenia Muscle. 2019 Apr;10(2):287-297. doi: 10.1002/jcsm.12382. Epub 2019 Mar 4.
Older adults with cancer experience negative long-term functional effects of both cancer and treatments. Exercise may minimize their age-related and cancer-related functional decline.
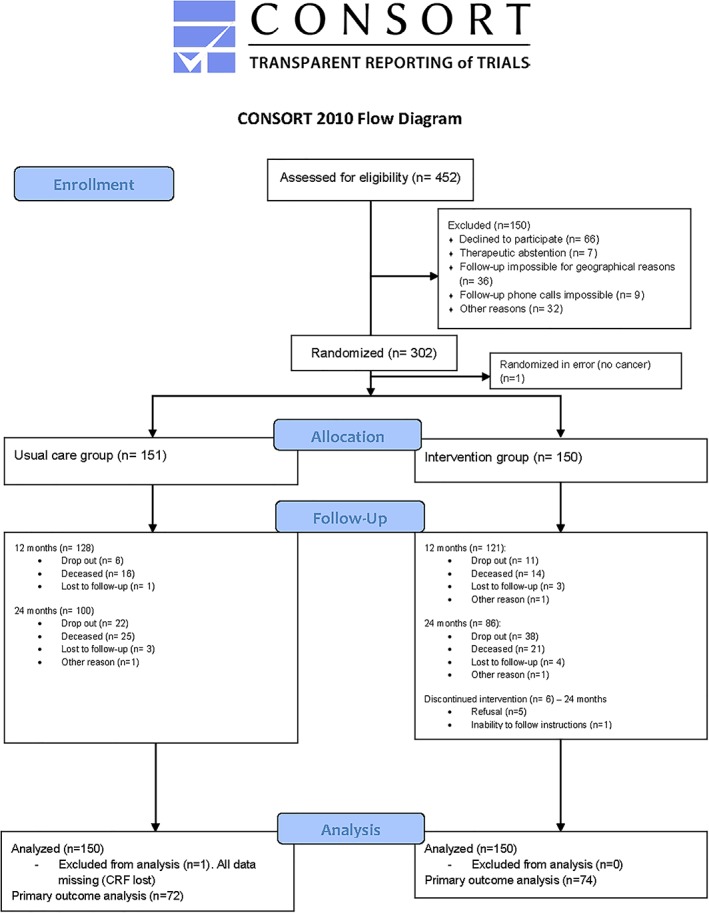
We conducted a multicentre open-label 12 month randomized clinical trial with two parallel arms including participants aged ≥70 years with lymphoma or carcinoma requiring curative treatment. The study started at the beginning of any phase of cancer treatment (surgery, chemotherapy, or radiotherapy). The usual care group (UCG) received the current national recommendations in physical activity (a guideline without specific counselling). The intervention group (IG) received 1 year phoned physical activity advice individually adapted to physical assessment (twice a month during the first 6 months and then monthly). The primary outcome was the proportion of subjects with a 1 year decreased short physical performance battery (SPPB) score of 1 point or more. Physical, cognitive, and clinical secondary outcomes were also investigated.
We allocated 301 participants (age 76.7 ± 5.0, female 60.6%) to each group. At baseline, the median SPPB was 10/12 in both groups. Breast was the most frequent tumour site (35.7%). After 1 year, 14.0% of participants in the UCG and 18.7% in the IG had a decrease in SPPB score of 1 point or more (P = 0.772). At 2 years, there was no difference in SPPB, gait speed, International Physical Activity Questionnaire score, and verbal fluency. Subgroup analyses after 2 years showed a decline in SPPB for 29.8% of UCG and 5.0% of IG breast cancer participants (P = 0.006), in 21.7% of UCG and 6.2% of IG female participants (P = 0.019), and in 24.5% of UCG and 11.1% of IG normal nutritional status participants (P = 0.009). Falls, hospitalization, institutionalization, and death rates were similar in both groups.
Personalized phoned physical activity advice had not reduced functional decline at 1 year but provided preliminary evidence that may prevent physical performance decline at 2 years in older adults with breast cancer.
患有癌症的老年人会经历癌症及其治疗带来的负面长期功能影响。运动可能会最小化他们与年龄相关和与癌症相关的功能下降。
我们开展了一项多中心、开放标签、12 个月随机临床试验,设有两个平行组,纳入年龄≥70 岁、需要根治性治疗的淋巴瘤或癌患者。研究开始于癌症治疗的任何阶段(手术、化疗或放疗)。常规治疗组(UCG)接受目前国家推荐的体力活动(没有具体咨询的指南)。干预组(IG)接受为期 1 年的个性化电话体力活动咨询,根据身体评估进行调整(前 6 个月每月两次,然后每月一次)。主要结局是 1 年内短体适能表现电池(SPPB)评分下降 1 分或更多的患者比例。还调查了身体、认知和临床次要结局。
我们将 301 名参与者(年龄 76.7±5.0,女性 60.6%)分配到每组。在基线时,两组的 SPPB 中位数均为 10/12。乳腺癌是最常见的肿瘤部位(35.7%)。1 年后,UCG 组有 14.0%的参与者和 IG 组有 18.7%的参与者 SPPB 评分下降 1 分或更多(P=0.772)。在 2 年时,SPPB、步态速度、国际体力活动问卷评分和言语流畅性无差异。2 年后的亚组分析显示,UCG 组有 29.8%的乳腺癌参与者和 IG 组有 5.0%的参与者 SPPB 下降(P=0.006),UCG 组有 21.7%的女性参与者和 IG 组有 6.2%的女性参与者 SPPB 下降(P=0.019),UCG 组有 24.5%的正常营养状态参与者和 IG 组有 11.1%的正常营养状态参与者 SPPB 下降(P=0.009)。两组的跌倒、住院、住院和死亡率相似。
个性化电话体力活动咨询并未在 1 年内减少功能下降,但提供了初步证据,表明可能预防 2 年内老年乳腺癌患者的身体表现下降。