School of Applied Sciences, State University of Campinas (UNICAMP), Limeira 13484-350 SP, Brazil.
Department of Internal Medicine, State University of Campinas (UNICAMP), Campinas 13083-887 SP, Brazil.
Nutrients. 2019 Mar 1;11(3):536. doi: 10.3390/nu11030536.
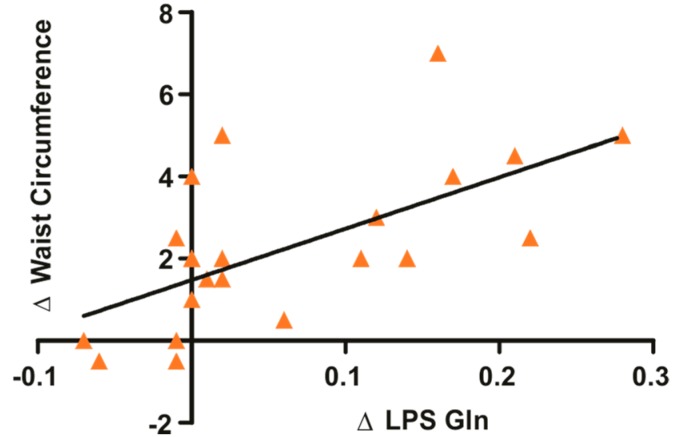
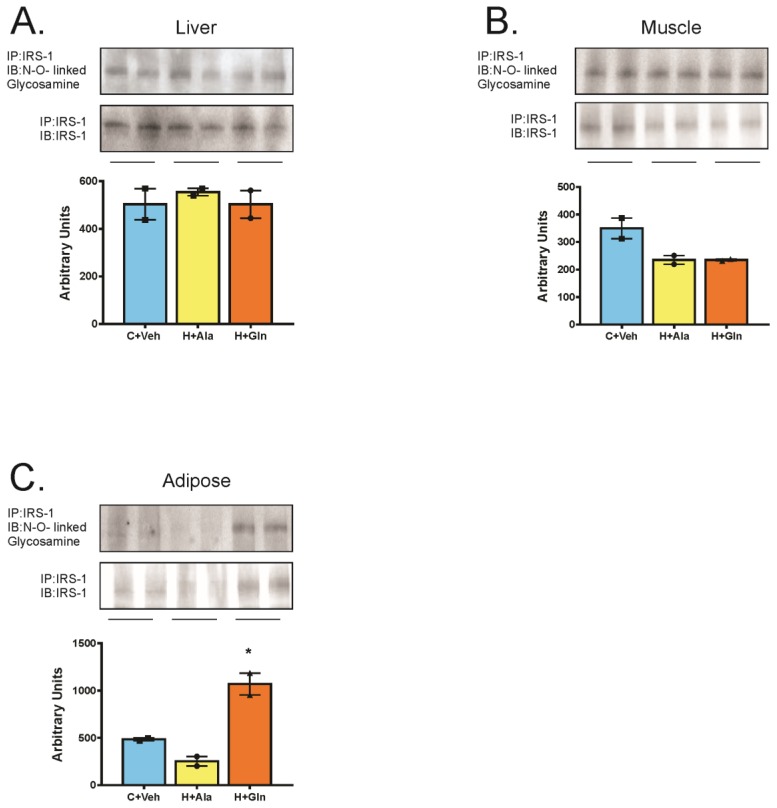
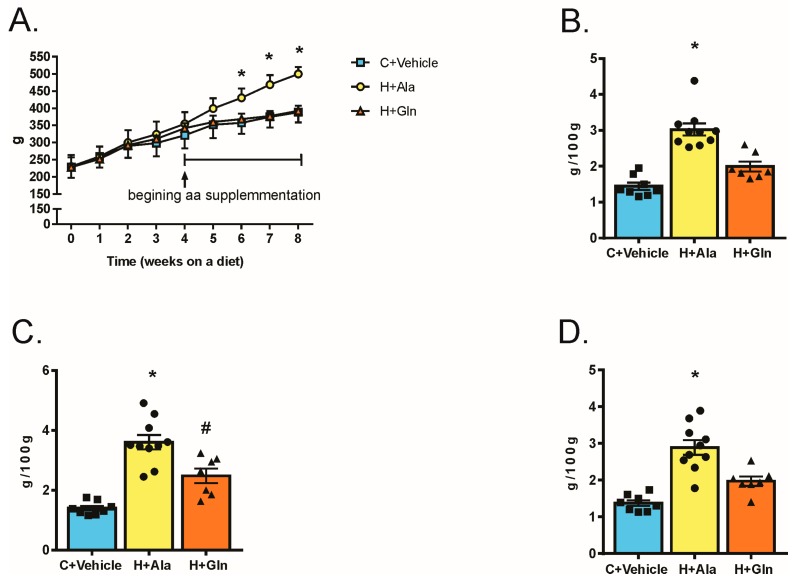
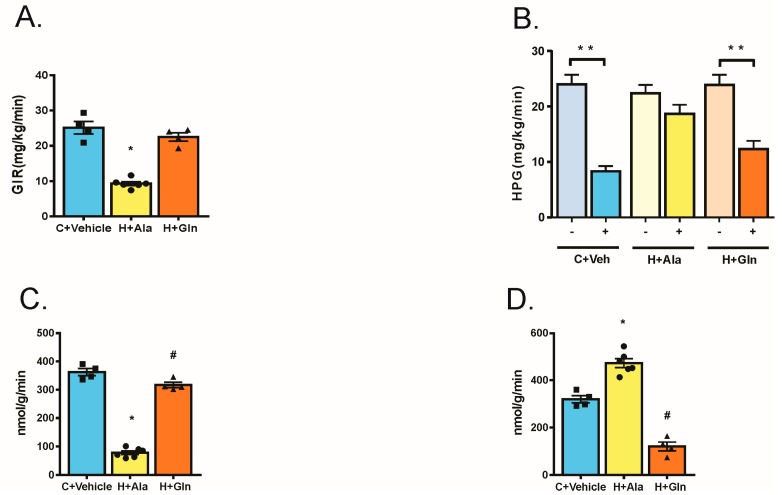
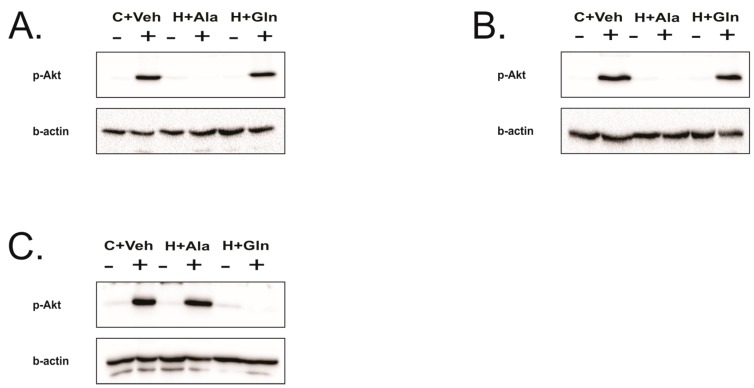
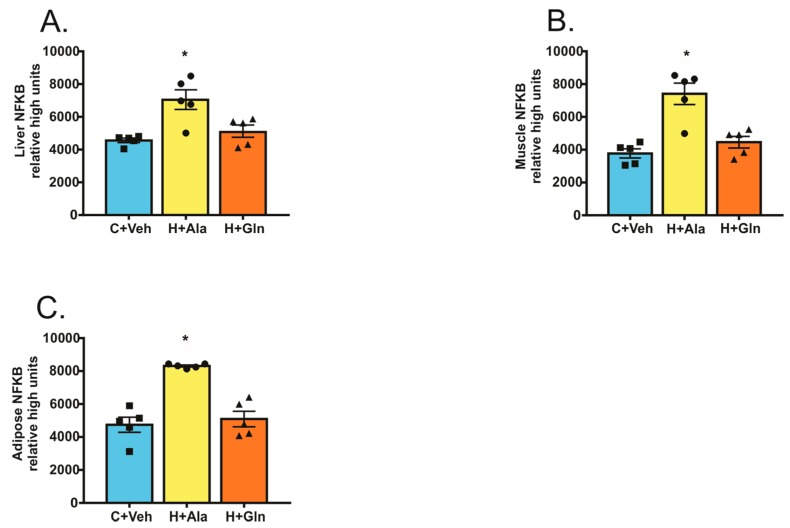
In the present study, we aimed to investigate whether chronic oral glutamine (Gln) supplementation may alter metabolic parameters and the inflammatory profile in overweight and obese humans as well as whether Gln may modulate molecular pathways in key tissues linked to the insulin action in rats. Thirty-nine overweight/obese volunteers received 30 g of Gln or alanine (Ala-control) for 14 days. Body weight (BW), waist circumference (WC), hormones, and pro-inflammatory markers were evaluated. To investigate molecular mechanisms, Gln or Ala was given to Wistar rats on a high-fat diet (HFD), and metabolic parameters, euglycemic hyperinsulinemic clamp with tracers, and Western blot were done. Gln reduced WC and serum lipopolysaccharide (LPS) in overweight volunteers. In the obese group, Gln diminished WC and serum insulin. There was a positive correlation between the reduction on WC and LPS. In rats on HFD, Gln reduced adiposity, improved insulin action and signaling, and reversed both defects in glucose metabolism in the liver and muscle. Gln supplementation increased muscle glucose uptake and reversed the increased hepatic glucose production, in parallel with a reduced glucose uptake in adipose tissue. This insulin resistance in AT was accompanied by enhanced IRS1 O-linked-glycosamine association in this tissue, but not in the liver and muscle. These data suggest that Gln supplementation leads to insulin resistance specifically in adipose tissue via the hexosamine pathway and reduces adipose mass, which is associated with improvement in the systemic insulin action. Thus, further investigation with Gln supplementation should be performed for longer periods in humans before prescribing as a beneficial therapeutic approach for individuals who are overweight and obese.
在本研究中,我们旨在研究慢性口服谷氨酰胺(Gln)补充是否可以改变超重和肥胖人群的代谢参数和炎症特征,以及 Gln 是否可以调节与大鼠胰岛素作用相关的关键组织中的分子途径。39 名超重/肥胖志愿者接受 30 克 Gln 或丙氨酸(Ala-对照)治疗 14 天。评估体重(BW)、腰围(WC)、激素和促炎标志物。为了研究分子机制,将 Gln 或 Ala 给予高脂肪饮食(HFD)的 Wistar 大鼠,并进行代谢参数、正葡萄糖高胰岛素钳夹和 Western blot。Gln 可降低超重志愿者的 WC 和血清脂多糖(LPS)。在肥胖组中,Gln 降低了 WC 和血清胰岛素。WC 和 LPS 的减少呈正相关。在 HFD 大鼠中,Gln 降低了肥胖度,改善了胰岛素作用和信号转导,并逆转了肝脏和肌肉中葡萄糖代谢的缺陷。Gln 补充增加了肌肉葡萄糖摄取,并逆转了肝葡萄糖生成的增加,同时脂肪组织的葡萄糖摄取减少。这种脂肪组织中的胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种脂肪组织中的胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种脂肪组织中的胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。这种胰岛素抵抗伴随着 IRS1 O-连接氨基葡萄糖结合的增加,但在肝脏和肌肉中没有增加。