Institute of Infection and Global Health, University of Liverpool, 8 West Derby St, Liverpool, L69 7BE, UK.
Infectious Diseases Department, Alder Hey Children's NHS Foundation Trust, Eaton Road, Liverpool, L12 2AP, UK.
BMC Med. 2019 Mar 6;17(1):48. doi: 10.1186/s12916-019-1275-z.
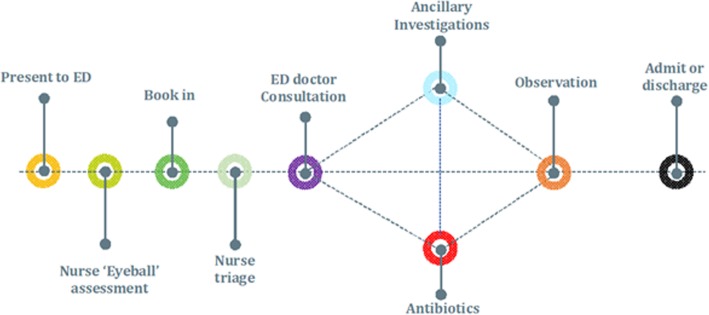
Paediatric fever is a common cause of emergency department (ED) attendance. A lack of prompt and definitive diagnostics makes it difficult to distinguish viral from potentially life-threatening bacterial causes, necessitating a cautious approach. This may result in extended periods of observation, additional radiography, and the precautionary use of antibiotics (ABs) prior to evidence of bacterial foci. This study examines resource use, service costs, and health outcomes.
We studied an all-year prospective, comprehensive, and representative cohort of 6518 febrile children (aged < 16 years), attending Alder Hey Children's Hospital, an NHS-affiliated paediatric care provider in the North West of England, over a 1-year period. Performing a time-driven and activity-based micro-costing, we estimated the economic impact of managing paediatric febrile illness, with focus on nurse/clinician time, investigations, radiography, and inpatient stay. Using bootstrapped generalised linear modelling (GLM, gamma, log), we identified the patient and healthcare provider characteristics associated with increased resource use, applying retrospective case-note identification to determine rates of potentially avoidable AB prescribing.
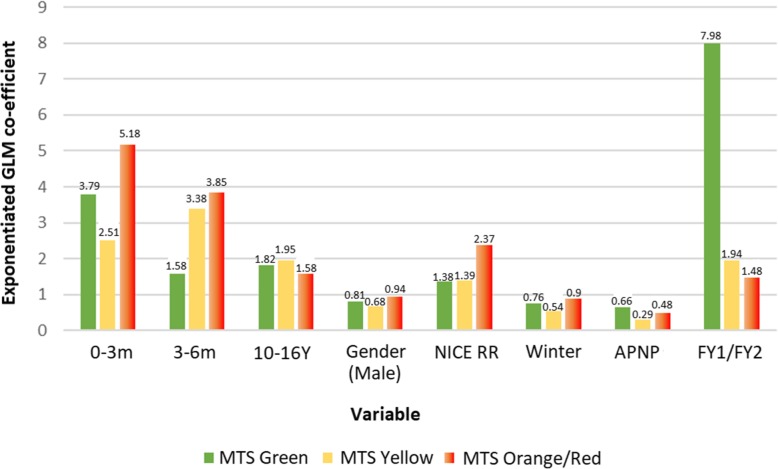
Infants aged less than 3 months incurred significantly higher resource use than any other age group, at £1000.28 [95% CI £82.39-£2993.37] per child, (p < 0.001), while lesser experienced doctors exhibited 3.2-fold [95% CI 2.0-5.1-fold] higher resource use than consultants (p < 0.001). Approximately 32.4% of febrile children received antibiotics, and 7.1% were diagnosed with bacterial infections. Children with viral illnesses for whom antibiotic prescription was potentially avoidable incurred 9.9-fold [95% CI 6.5-13.2-fold] cost increases compared to those not receiving antibiotics, equal to an additional £1352.10 per child, predominantly resulting from a 53.9-h increase in observation and inpatient stay (57.1 vs. 3.2 h). Bootstrapped GLM suggested that infants aged below 3 months and those prompting a respiratory rate 'red flag', treatment by lesser experienced doctors, and Manchester Triage System (MTS) yellow or higher were statistically significant predictors of higher resource use in 100% of bootstrap simulations.
The economic impact of diagnostic uncertainty when managing paediatric febrile illness is significant, and the precautionary use of antibiotics is strongly associated with increased costs. The use of ED resources is highest among infants (aged less than 3 months) and those infants managed by lesser experienced doctors, independent of clinical severity. Diagnostic advances which could increase confidence to withhold antibiotics may yield considerable efficiency gains in these groups, where the perceived risks of failing to identify potentially life-threatening bacterial infections are greatest.
儿科发热是急诊科(ED)就诊的常见原因。由于缺乏及时和明确的诊断,难以区分病毒性和潜在危及生命的细菌性病因,因此需要谨慎处理。这可能导致观察时间延长、额外的放射检查,并在出现细菌性病灶之前预防性使用抗生素(ABs)。本研究考察了资源利用、服务成本和健康结果。
我们研究了一个全年、全面和具有代表性的队列,该队列包括 6518 名发热儿童(年龄<16 岁),他们在英格兰西北部的 NHS 附属儿科护理机构 Alder Hey 儿童医院就诊,时间为 1 年。通过时间驱动和基于活动的微观成本核算,我们估计了管理儿科发热性疾病的经济影响,重点是护士/临床医生的时间、检查、放射检查和住院时间。使用 bootstrap 广义线性建模(GLM,伽马,对数),我们确定了与资源利用增加相关的患者和医疗服务提供者特征,并通过回顾性病例记录识别确定了潜在可避免 AB 处方的发生率。
年龄小于 3 个月的婴儿比任何其他年龄组的资源利用率都高,每位儿童的费用为 1000.28 英镑[95%置信区间(CI)82.39-2993.37 英镑](p<0.001),而经验较少的医生的资源利用率比顾问高 3.2 倍[95% CI 2.0-5.1 倍](p<0.001)。约 32.4%的发热儿童接受了抗生素治疗,7.1%被诊断为细菌感染。对于病毒性疾病患者,如果抗生素处方可以避免,与未接受抗生素治疗的患者相比,成本增加了 9.9 倍[95% CI 6.5-13.2 倍],相当于每位儿童额外增加 1352.10 英镑,主要是由于观察和住院时间增加了 53.9 小时(57.1 小时与 3.2 小时)。Bootstrap GLM 表明,年龄小于 3 个月的婴儿和提示呼吸频率“红色标记”的婴儿、经验较少的医生治疗的婴儿,以及曼彻斯特分诊系统(MTS)黄色或更高的婴儿是资源利用率增加的统计学显著预测因素,在 100%的 bootstrap 模拟中均如此。
在管理儿科发热性疾病时,诊断不确定性的经济影响是巨大的,而预防性使用抗生素与成本增加密切相关。急诊科资源的使用在婴儿(<3 个月)和经验较少的医生治疗的婴儿中最高,独立于临床严重程度。能够提高对不使用抗生素的信心的诊断进展可能会在这些群体中带来相当大的效率提高,因为在这些群体中,未能识别潜在危及生命的细菌感染的风险被认为最大。