de Montigny Simon, Boily Marie-Claude, Mâsse Benoît R, Mitchell Kate M, Dimitrov Dobromir T
CHU Sainte-Justine Research Center, Montreal, QC, Canada.
School of Public Health, University of Montreal, Montreal, QC, Canada.
Infect Dis Model. 2018 Mar 14;3:85-96. doi: 10.1016/j.idm.2018.03.005. eCollection 2018.
The epidemiological tipping point ratio (TPR) has been suggested as a useful indicator to monitor the scale-up of antiretroviral treatment (ART) programmes and determine when scale-up is sufficient to control the epidemic. TPR has been defined as the ratio of yearly number of new HIV infections to the yearly number of new ART initiations or to the yearly net increase in the number of people on ART. It has been used to rank the progress of treatment programmes across countries, with the objective of reaching a TPR value under 1. Our study aims to assess if TPR alone can be used as an indicator of ART success across settings by comparing the expected changes in HIV incidence and ART coverage when TPR is maintained constant over time. In particular, we focus on the effect of ART initiation timing (emphasis on ART being initiated early or late during HIV progression) on the interpretation of the TPR.
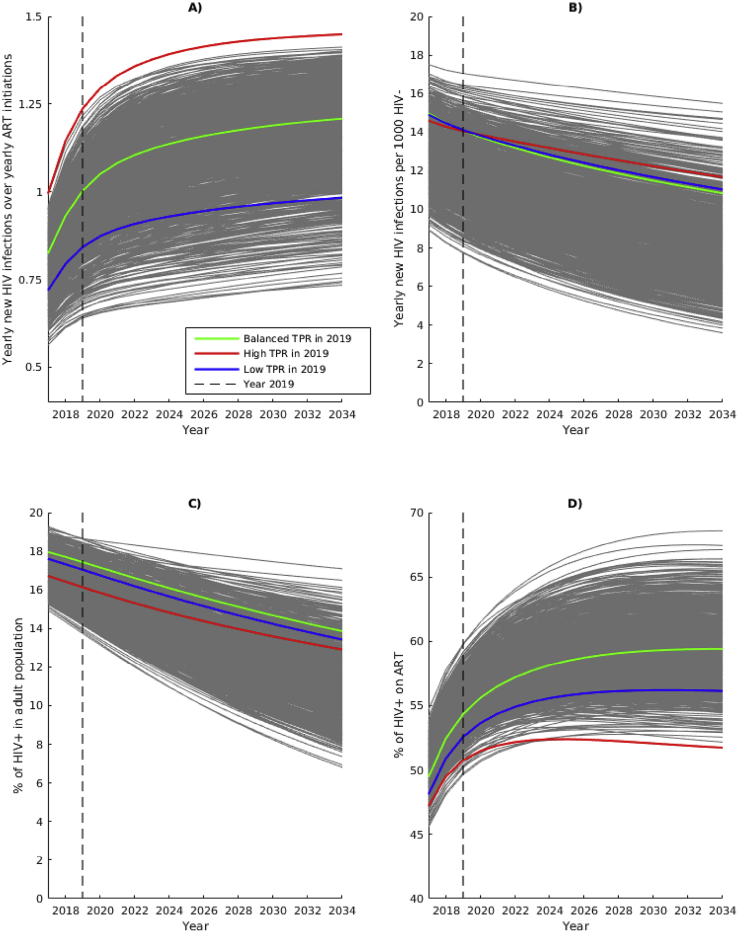
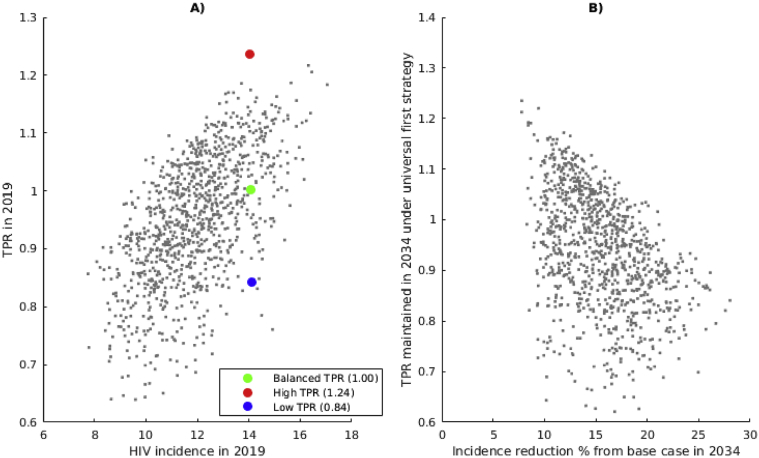
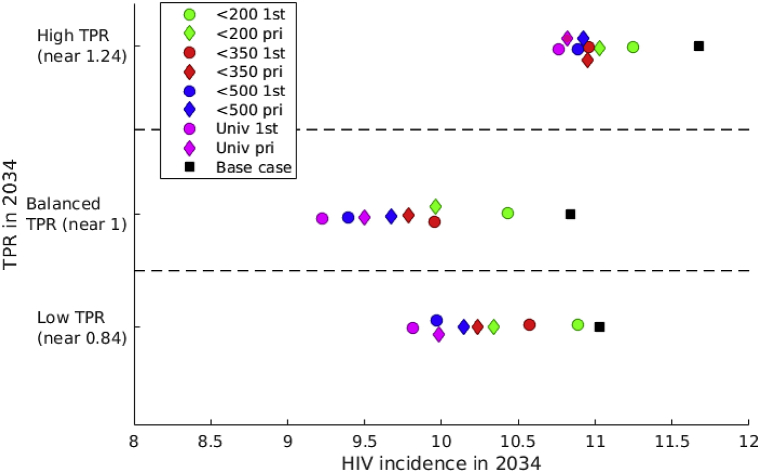
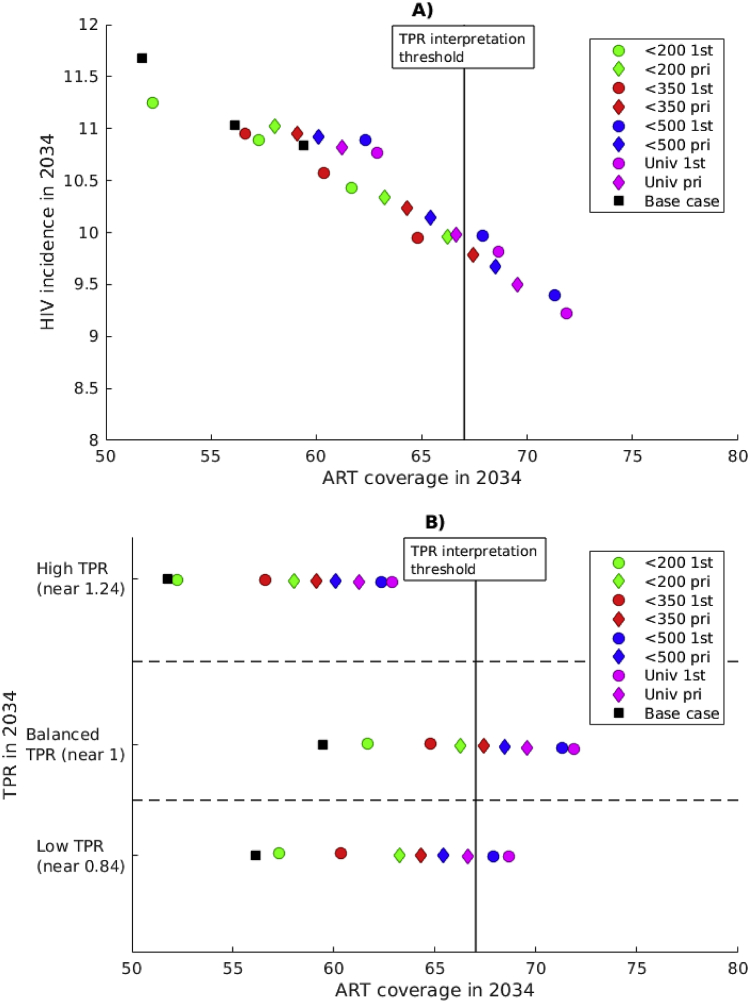
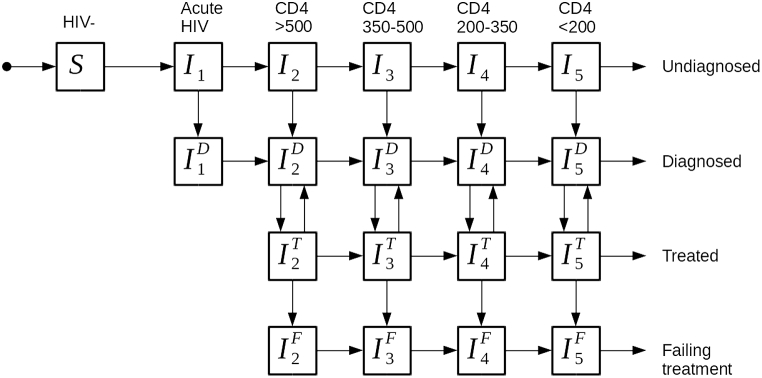
We used a dynamic model of HIV transmission in South Africa representing ART rollout leading to universal treatment in 2017. The model is calibrated to HIV incidence, HIV prevalence and ART coverage in 2012 in South Africa, and 1000 simulations are selected for the base-case scenario. To measure the effect of TPR, we simulate TPR-preserving interventions, maintaining TPR (yearly number of new ART initiations denominator) at the value observed in 2019 (between 0.65 and 1.25) for 15 years. We compare ART coverage and HIV incidence across TPR values and across strategies in which ART access is prioritized differently. In a secondary analysis, we illustrate the sensitivity of new ART initiations to ART retention, and we compare both definitions of the TPR.
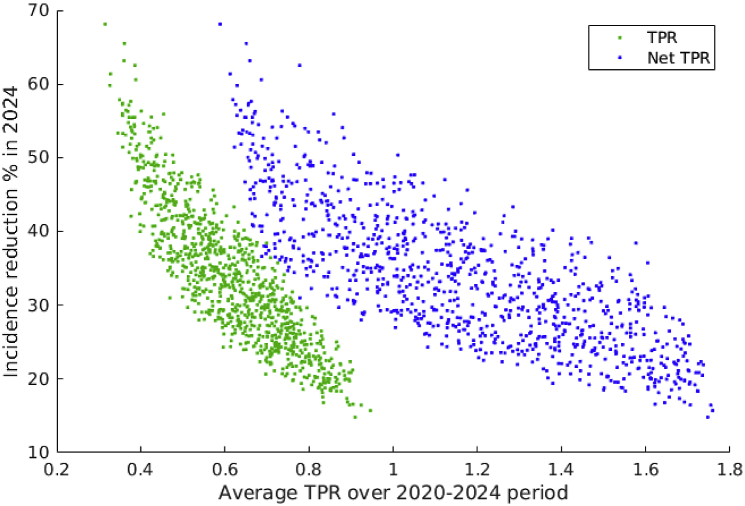
Our analysis shows that HIV incidence reduction is weakly correlated to TPR: the same reduction in HIV incidence (15%) can be achieved by implementing the same strategy with a wide range of TPR maintained (0.65-1.12). Assuming high retention in ART, TPR-preserving strategies prioritizing early ART initiation yield greater reduction in HIV incidence than strategies where most individuals initiate ART late. High ART coverage is associated with low HIV incidence and it can be reached with a TPR below or equal to one with strategies favoring early ART initiation. Low ART retention over time results in higher HIV incidence even if TPR is maintained low. If ART retention is low, strategies prioritizing late ART initiation are associated with lower HIV incidence than strategies where ART is initiated early. Maintaining a fixed TPR value based on the net increase in people on ART gives higher HIV incidence reduction and requires fast ART scale-up.
Our analysis suggests that the TPR is not an adequate indicator of ART programme impact, without information on ART coverage and retention. Achieving early initiation and adherence to treatment to improve ART coverage might be as important as attaining a specific TPR target. Comparisons of TPR in different settings should account for differences in epidemic conditions.
流行病学临界点比率(TPR)被认为是监测抗逆转录病毒治疗(ART)项目扩大规模以及确定扩大规模何时足以控制疫情的有用指标。TPR被定义为每年新感染艾滋病毒的人数与每年开始接受抗逆转录病毒治疗的新人数或每年接受抗逆转录病毒治疗人数的净增加数之比。它已被用于对各国治疗项目的进展进行排名,目标是使TPR值低于1。我们的研究旨在通过比较当TPR随时间保持恒定时艾滋病毒发病率和抗逆转录病毒治疗覆盖率的预期变化,评估仅TPR是否可作为不同环境下抗逆转录病毒治疗成功的指标。特别是,我们关注抗逆转录病毒治疗启动时间(强调在艾滋病毒进展过程中抗逆转录病毒治疗是早启动还是晚启动)对TPR解释的影响。
我们使用了一个南非艾滋病毒传播动态模型,该模型代表了抗逆转录病毒治疗的推广,到2017年实现普遍治疗。该模型根据2012年南非的艾滋病毒发病率、艾滋病毒流行率和抗逆转录病毒治疗覆盖率进行校准,并为基线情景选择1000次模拟。为了衡量TPR的影响,我们模拟保持TPR的干预措施,将TPR(每年开始接受抗逆转录病毒治疗的新人数分母)保持在2019年观察到的值(0.65至1.25之间)15年。我们比较不同TPR值以及抗逆转录病毒治疗获取优先级不同的策略下的抗逆转录病毒治疗覆盖率和艾滋病毒发病率。在二次分析中,我们说明了新开始接受抗逆转录病毒治疗对治疗保留率的敏感性,并比较了TPR的两种定义。
我们的分析表明,艾滋病毒发病率的降低与TPR的相关性较弱:通过实施相同策略并保持广泛的TPR范围(0.65 - 1.12),可以实现相同的艾滋病毒发病率降低(15%)。假设抗逆转录病毒治疗保留率高,优先早期启动抗逆转录病毒治疗的保持TPR策略比大多数个体晚启动抗逆转录病毒治疗的策略能更大程度地降低艾滋病毒发病率。高抗逆转录病毒治疗覆盖率与低艾滋病毒发病率相关,通过优先早期启动抗逆转录病毒治疗的策略,TPR低于或等于1时即可实现高覆盖率。随着时间推移,抗逆转录病毒治疗保留率低会导致艾滋病毒发病率更高,即使TPR保持较低水平。如果抗逆转录病毒治疗保留率低,优先晚启动抗逆转录病毒治疗的策略比早启动抗逆转录病毒治疗的策略导致的艾滋病毒发病率更低。基于接受抗逆转录病毒治疗人数的净增加来维持固定的TPR值,可实现更大程度的艾滋病毒发病率降低,且需要快速扩大抗逆转录病毒治疗规模。
我们的分析表明,如果没有关于抗逆转录病毒治疗覆盖率和保留率的信息,TPR并非抗逆转录病毒治疗项目影响的充分指标。实现早期启动并坚持治疗以提高抗逆转录病毒治疗覆盖率可能与达到特定的TPR目标同样重要。不同环境下TPR的比较应考虑疫情状况的差异。