From the Department of Medicine (H.R., F.N., E.K.), Guthrie Health System/Robert Packer Hospital, Sayre, PA.
Department of Medicine, West Virginia University, Morgantown (S.U.K.).
Stroke. 2019 Apr;50(4):947-953. doi: 10.1161/STROKEAHA.118.023978.
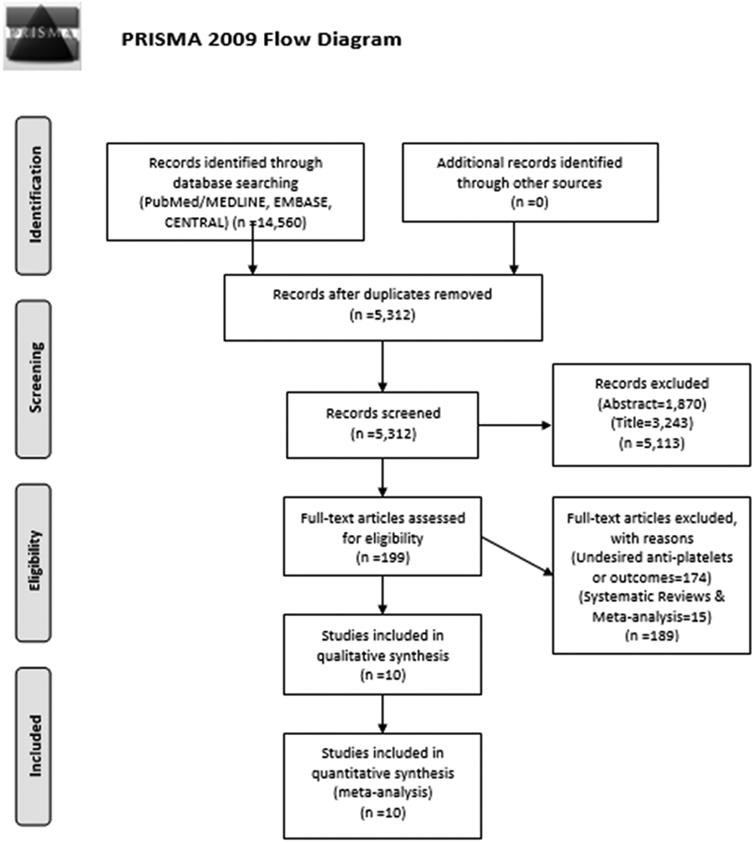
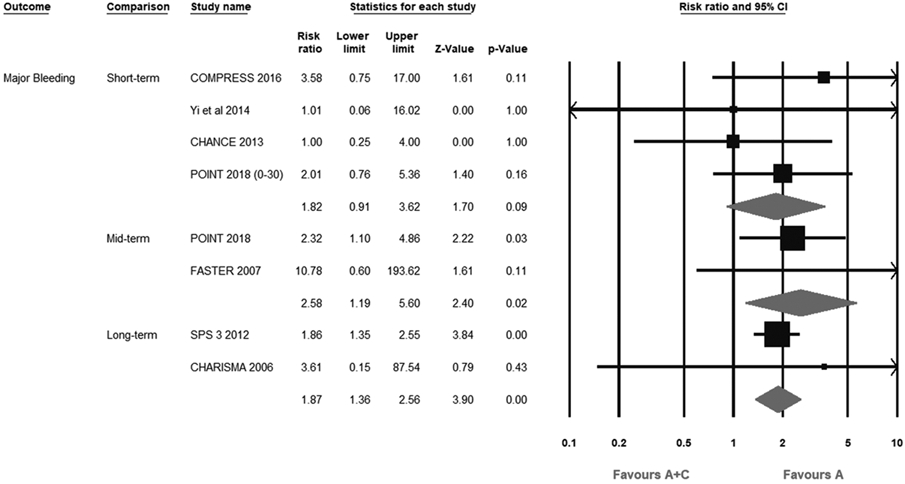
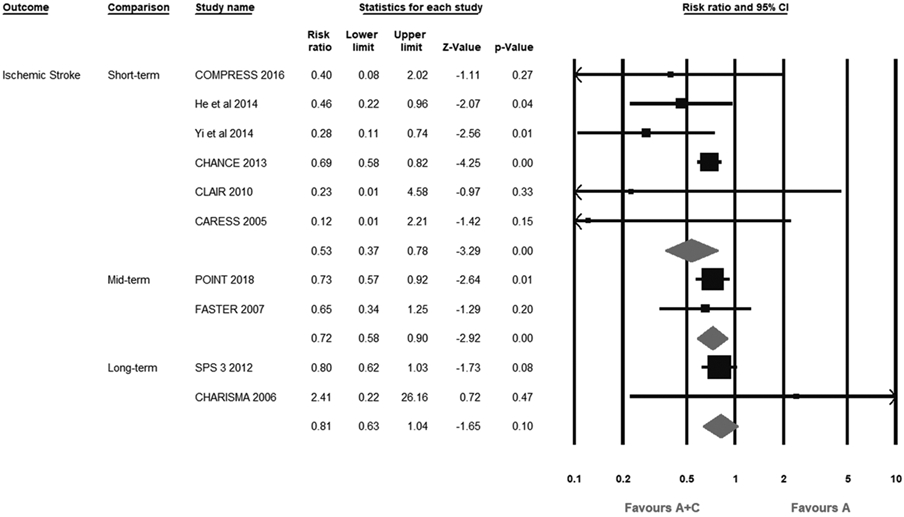
Background and Purpose- The role of aspirin plus clopidogrel (A+C) therapy compared with aspirin monotherapy in patients presenting with acute ischemic stroke (IS) or transient ischemic attack remains uncertain. We conducted this study to determine the optimal period of efficacy and safety of A+C compared with aspirin monotherapy. Methods- Ten randomized controlled trials (15 434 patients) were selected using MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) (inception June 2018) comparing A+C with aspirin monotherapy in patients with transient ischemic attack or IS. The primary efficacy outcome was recurrent IS, and the primary safety outcome was major bleeding. The secondary outcomes were major adverse cardiovascular events (composite of stroke, myocardial infarction, and cardiovascular mortality) and all-cause mortality. We stratified analysis based on the short- (≤1 month), intermediate- (≤3 month), and long-term (>3 month) A+C therapy. Effects were estimated as relative risk (RR) with 95% CI. Results- A+C significantly reduced the risk of recurrent IS at short-term (RR, 0.53; 95% CI, 0.37-0.78) and intermediate-term (RR, 0.72; 95% CI, 0.58-0.90) durations. Similarly, major adverse cardiovascular event was significantly reduced by short-term (RR, 0.68; 95% CI, 0.60-0.78) and intermediate-term (RR, 0.76; 95% CI, 0.61-0.94) A+C therapy. However, long-term A+C did not yield beneficial effect in terms of recurrent IS (RR, 0.81; 95% CI, 0.63-1.04) and major adverse cardiovascular events (RR, 0.87; 95% CI, 0.71-1.07). Intermediate-term (RR, 2.58; 95% CI, 1.19-5.60) and long-term (RR, 1.87; 95% CI, 1.36-2.56) A+C regimens significantly increased the risk of major bleeding as opposed to short-term A+C (RR, 1.82; 95% CI, 0.91-3.62). Excessive all-cause mortality was limited to long-term A+C (RR, 1.45; 95% CI, 1.10-1.93). Conclusions- Short-term A+C is more effective and equally safe in comparison to aspirin alone in patients with acute IS or transient ischemic attack.
背景与目的-在急性缺血性脑卒中(IS)或短暂性脑缺血发作(TIA)患者中,阿司匹林联合氯吡格雷(A+C)治疗与阿司匹林单药治疗相比,其作用尚不确定。我们进行了这项研究,以确定 A+C 与阿司匹林单药治疗相比的最佳疗效和安全性时间窗。
方法-我们使用 MEDLINE、EMBASE 和 Cochrane 对照试验中心注册库(CENTRAL)(截至 2018 年 6 月),检索了 10 项比较 TIA 或 IS 患者中 A+C 与阿司匹林单药治疗的随机对照试验(15434 例患者)。主要疗效结局为复发性 IS,主要安全性结局为大出血。次要结局为主要不良心血管事件(卒中、心肌梗死和心血管死亡率的复合结局)和全因死亡率。我们根据 A+C 治疗的短期(≤1 个月)、中期(≤3 个月)和长期(>3 个月)进行分层分析。采用相对风险(RR)及其 95%置信区间(CI)评估效应。
结果-A+C 可显著降低短期(RR,0.53;95%CI,0.37-0.78)和中期(RR,0.72;95%CI,0.58-0.90)A+C 治疗的复发性 IS 风险。同样,短期(RR,0.68;95%CI,0.60-0.78)和中期(RR,0.76;95%CI,0.61-0.94)A+C 治疗也显著降低了主要不良心血管事件的风险。然而,长期 A+C 治疗并未在复发性 IS(RR,0.81;95%CI,0.63-1.04)和主要不良心血管事件(RR,0.87;95%CI,0.71-1.07)方面产生获益。与短期 A+C 相比,中期(RR,2.58;95%CI,1.19-5.60)和长期(RR,1.87;95%CI,1.36-2.56)A+C 方案显著增加了大出血风险(RR,1.82;95%CI,0.91-3.62)。全因死亡率过高仅限于长期 A+C(RR,1.45;95%CI,1.10-1.93)。
结论-在急性 IS 或 TIA 患者中,短期 A+C 比阿司匹林单药治疗更有效且安全性相当。