Department of Biomedical Physiology and Kinesiology, Simon Fraser University, Burnaby, BC, V5A 1S6, Canada.
BMC Geriatr. 2019 Mar 13;19(1):80. doi: 10.1186/s12877-019-1082-6.
Orthostatic hypotension (OH; profound falls in blood pressure when upright) is a common deficit that increases in incidence with age, and may be associated with falling risk. Deficit accumulation results in frailty, regarded as enhanced vulnerability to adverse outcomes. We aimed to evaluate the relationships between OH, frailty, falling and mortality in elderly care home residents.
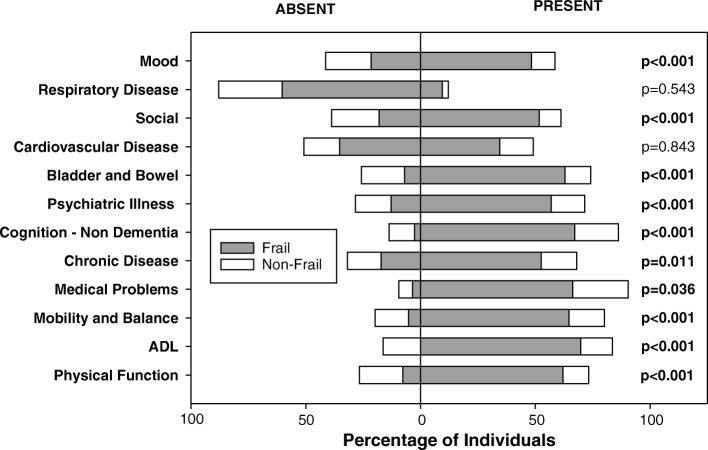
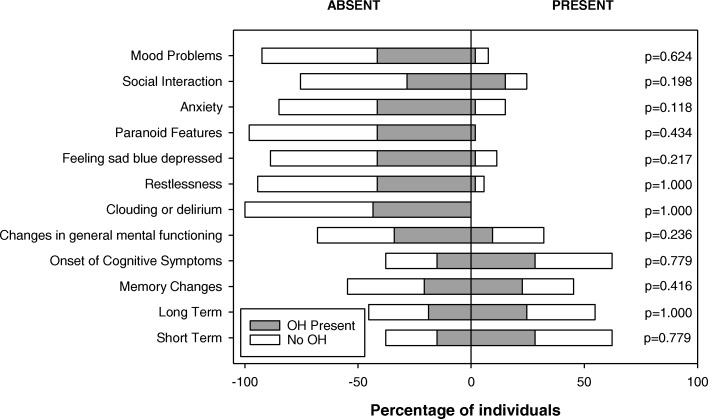
From the Minimum Data Set (MDS) document, a frailty index (FI-MDS) was generated from a list of 58 deficits, ranging from 0 (no deficits) to 1.0 (58 deficits). OH was evaluated from beat-to-beat blood pressure and heart rate (finger plethysmography) collected during a 15-min supine-seated orthostatic stress test. Retrospective and prospective falling rates (falls/year) were extracted from facility falls incident reports. All-cause 3-year mortality was determined. Data are reported as mean ± standard error.
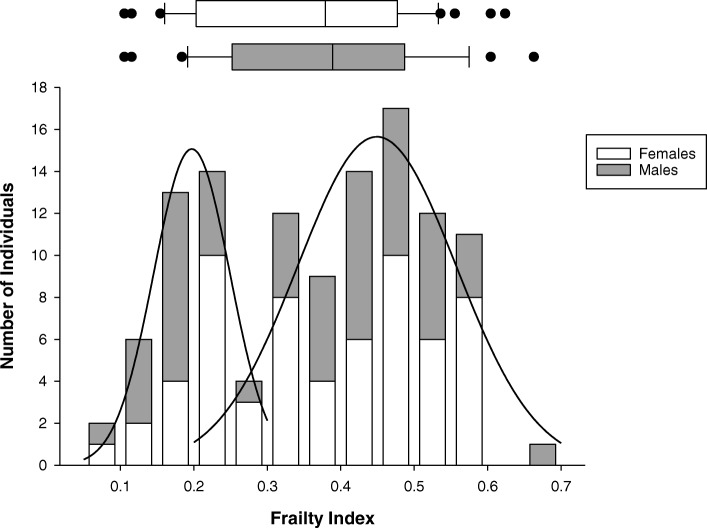
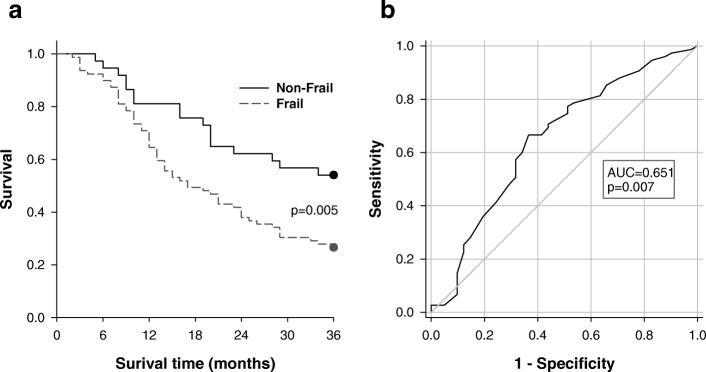
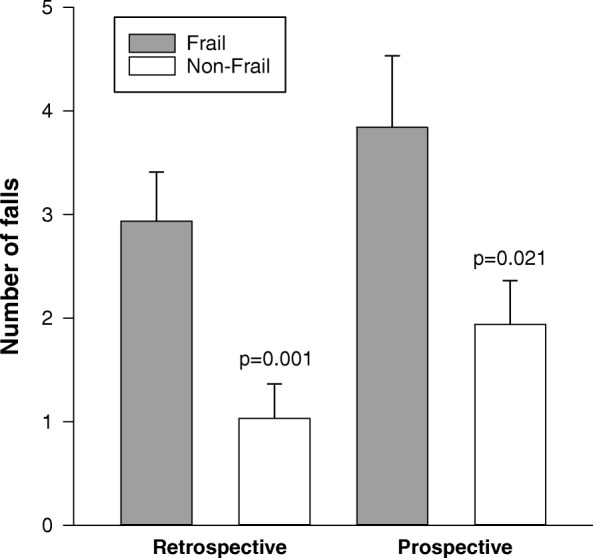
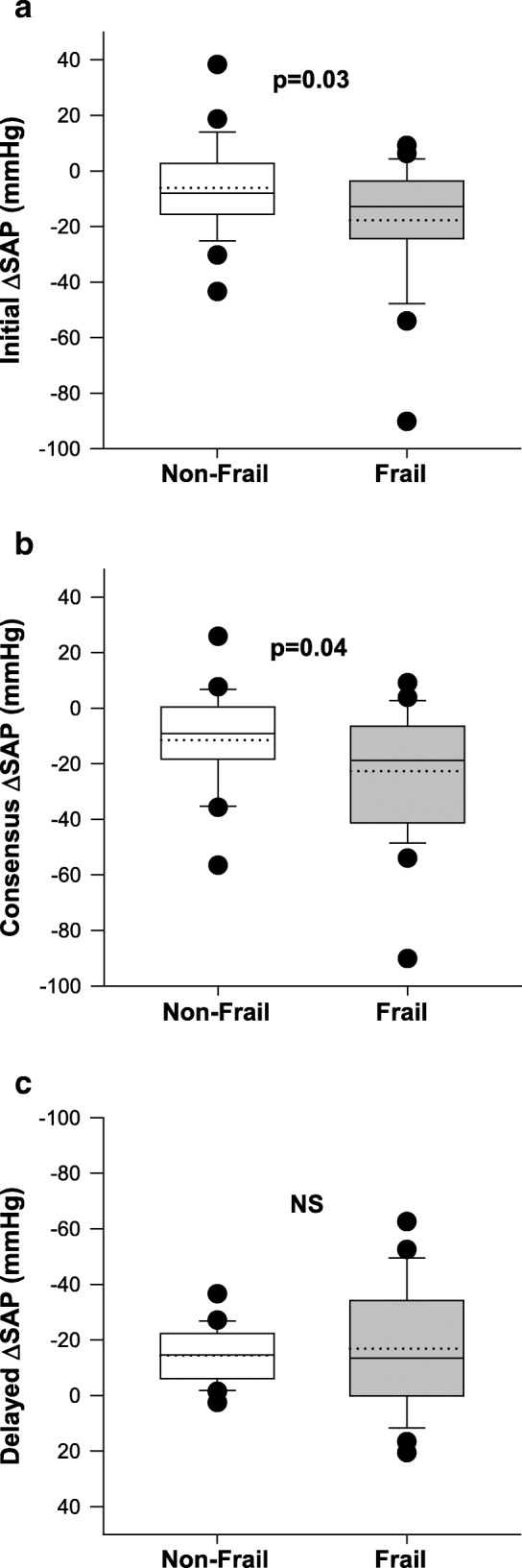
Data were obtained from 116 older adults (aged 84.2 ± 0.9 years; 44% males) living in two long term care facilities. The mean FI-MDS was 0.36 ± 0.01; FI-MDS was correlated with age (r = 0.277; p = 0.003). Those who were frail (FI ≥ 0.27) had larger Initial (- 17.8 ± 4.2 vs - 6.1 ± 3.3 mmHg, p = 0.03) and Consensus (- 22.7 ± 4.3 vs - 11.5 ± 3.3 mmHg, p = 0.04) orthostatic reductions in systolic arterial pressure. Frail individuals had higher prospective and retrospective falling rates and higher 3-year mortality. Receiver operating characteristic curves evaluated the ability of FI-MDS alone to predict prospective falls (sensitivity 72%, specificity 36%), Consensus OH (sensitivity 68%, specificity 60%) and 3-year mortality (sensitivity 77%, specificity 49%). Kaplan Meier survival analyses showed significantly higher 3-year mortality in those who were frail compared to the non-frail (p = 0.005).
Frailty can be captured using a frailty index based on MDS data in elderly individuals living in long term care, and is related to susceptibility to orthostatic hypotension, falling risk and 3-year mortality. Use of the MDS to generate a frailty index may represent a simple and convenient risk assessment tool for older adults living in long term care. Older adults who are both frail and have impaired orthostatic blood pressure control have a particularly high risk of falling and should receive tailored management to mitigate this risk.
直立性低血压(OH;当直立时血压明显下降)是一种常见的缺陷,随着年龄的增长发病率增加,并且可能与跌倒风险相关。缺陷的积累导致虚弱,被认为是对不良后果的易感性增强。我们旨在评估老年人护理院居民的 OH、虚弱、跌倒和死亡率之间的关系。
从最低数据集中(MDS)的文件中,根据 58 项缺陷列表生成虚弱指数(FI-MDS),范围从 0(无缺陷)到 1.0(58 项缺陷)。通过在 15 分钟仰卧位至坐姿的直立压力测试期间收集的逐搏血压和心率(手指体积描记法)来评估 OH。从设施跌倒事故报告中提取回顾性和前瞻性跌倒率(每年跌倒次数)。确定所有原因的 3 年死亡率。数据以平均值±标准误差表示。
从两家长期护理机构的 116 名老年人(年龄 84.2±0.9 岁;44%为男性)中获得了数据。平均 FI-MDS 为 0.36±0.01;FI-MDS 与年龄呈正相关(r=0.277;p=0.003)。虚弱的人(FI≥0.27)初始(-17.8±4.2 对-6.1±3.3mmHg,p=0.03)和共识(-22.7±4.3 对-11.5±3.3mmHg,p=0.04)收缩压的直立性降低更大。虚弱的人有更高的前瞻性和回顾性跌倒率和更高的 3 年死亡率。受试者工作特征曲线评估了 FI-MDS 单独预测前瞻性跌倒的能力(灵敏度 72%,特异性 36%)、共识 OH(灵敏度 68%,特异性 60%)和 3 年死亡率(灵敏度 77%,特异性 49%)。Kaplan-Meier 生存分析显示,虚弱的人 3 年死亡率明显高于非虚弱的人(p=0.005)。
可以使用基于 MDS 数据的虚弱指数来捕获老年人长期护理中的虚弱,并且与直立性低血压、跌倒风险和 3 年死亡率有关。使用 MDS 生成虚弱指数可能是评估长期护理老年人风险的一种简单方便的工具。虚弱且直立血压控制受损的老年人跌倒风险特别高,应进行针对性管理以降低这种风险。