Department of Geriatric Medicine, Oslo University Hospital, Ullevål, P. O Box 4956 Nydalen, 0424, Oslo, Norway.
Institute of Health and Society and Research Center for Habilitation and Rehabilitation Services and Models (CHARM), University of Oslo, P.O. Box 1130 Blindern, 0318, Oslo, Norway.
BMC Med Res Methodol. 2019 Mar 15;19(1):59. doi: 10.1186/s12874-019-0694-z.
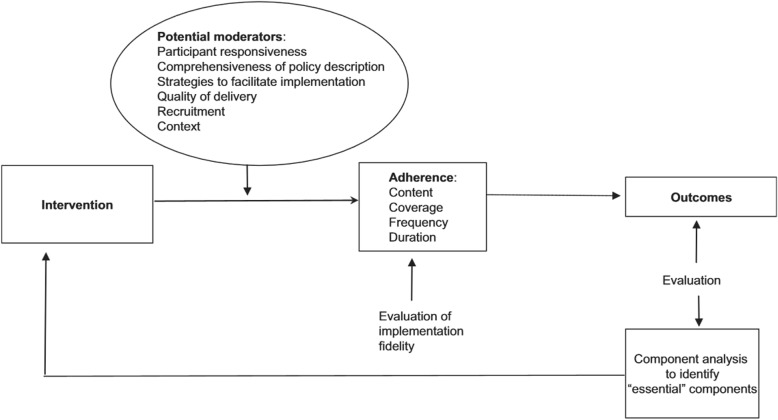
Evaluation of complex interventions should include a process evaluation to give evaluators, researchers, and policy makers greater confidence in the outcomes reported from RCTs. Implementation fidelity can be part of a process evaluation and refers to the degree to which an intervention is delivered according to protocol. The aim of this implementation fidelity study was to evaluate to what extent a dialogue-based psychosocial intervention was delivered according to protocol. A modified conceptual framework for implementation fidelity was used to guide the analysis.
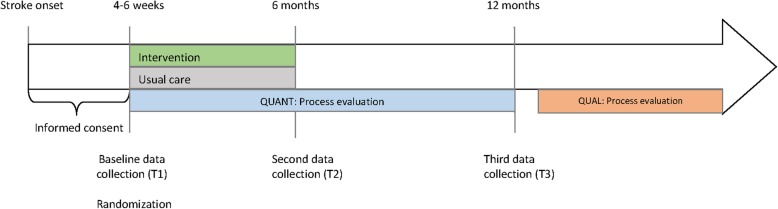
This study has an explanatory, sequential two-phase mixed methods design. Quantitative process data were collected longitudinally along with data collection in the RCT. Qualitative process data were collected after the last data collection point of the RCT. Descriptive statistical analyses were conducted to describe the sample, the intervention trajectories, and the adherence measures. A scoring system to clarify quantitative measurement of the levels of implementation was constructed. The qualitative data sources were analyzed separately with a theory-driven content analysis using categories of adherence and potential moderating factors identified in the conceptual framework of implementation fidelity. The quantitative adherence results were extended with the results from the qualitative analysis to assess which potential moderators may have influenced implementation fidelity and in what way.
The results show that the core components of the intervention were delivered although the intervention trajectories were individualized. Based on the composite score of adherence, results show that 80.1% of the interventions in the RCT were implemented with high fidelity. Although it is challenging to assess the importance of each of the moderating factors in relation to the other factors and to their influence on the adherence measures, participant responsiveness, comprehensiveness of policy description, context, and recruitment appeared to be the most prominent moderating factors of implementation fidelity in this study.
This evaluation of implementation fidelity and the discussion of what constitutes high fidelity implementation of this intervention are crucial in understanding the factors influencing the trial outcome. The study also highlights important methodological considerations for researchers planning process evaluations and studies of implementation fidelity.
ClinicalTrials.gov , NCT02338869; registered 10/04/2014.
评价复杂干预措施应包括一个过程评估,以让评估人员、研究人员和决策者对 RCT 报告的结果更有信心。实施保真度可以作为过程评估的一部分,是指干预措施按照方案实施的程度。本实施保真度研究旨在评估基于对话的心理社会干预措施在多大程度上按照方案实施。采用了修改后的实施保真度概念框架来指导分析。
本研究采用解释性、顺序两阶段混合方法设计。定量过程数据与 RCT 数据收集同时进行纵向收集。定性过程数据在 RCT 的最后一个数据收集点之后收集。描述性统计分析用于描述样本、干预轨迹和依从性测量。构建了一个评分系统,以澄清实施水平的定量测量。对定性数据来源进行了单独分析,使用在实施保真度概念框架中确定的依从性和潜在调节因素的类别进行理论驱动的内容分析。对定量依从性结果进行扩展,以评估潜在的调节因素可能如何影响实施保真度。
结果表明,尽管干预轨迹是个体化的,但干预的核心内容得到了实施。基于依从性的综合评分,结果显示 RCT 中有 80.1%的干预措施以高保真度实施。虽然评估每个调节因素相对于其他因素及其对依从性测量的影响的重要性具有挑战性,但参与者的反应性、政策描述的全面性、背景和招募似乎是本研究中实施保真度的最突出的调节因素。
对实施保真度的评估以及对构成这种干预高保真度实施的因素的讨论,对于理解影响试验结果的因素至关重要。该研究还强调了研究人员计划过程评估和实施保真度研究的重要方法学考虑因素。
ClinicalTrials.gov,NCT02338869;注册于 2014 年 10 月 4 日。