Department of Surgery, Division of Surgical Oncology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Department of Surgery, Division of Surgical Oncology, Catharina Hospital Eindhoven, Eindhoven, The Netherlands.
Ann Surg Oncol. 2019 Jul;26(7):2210-2221. doi: 10.1245/s10434-019-07294-y. Epub 2019 Mar 15.
Careful selection of patients with colorectal peritoneal metastases (PM) for cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is crucial. It remains unknown whether the time of onset of colorectal PM (synchronous vs metachronous) influences surgical morbidity and survival outcomes after CRS with HIPEC.
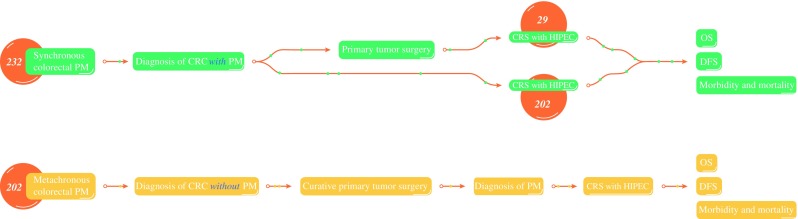
Patients with histologically proven colorectal PM who underwent CRS with HIPEC between February 2006 and December 2017 in two Dutch tertiary referral hospitals were retrospectively included from a prospectively maintained database. The onset of colorectal PM was classified as synchronous (PM diagnosed at the initiational presentation with colorectal cancer) or metachronous (PM diagnosed after initial curative colorectal resection). Major postoperative complications (Clavien-Dindo grade ≥ 3), overall survival (OS), and disease-free survival (DFS) were compared between patients with synchronous colorectal PM and those with metachronous colorectal PM using Kaplan-Meier analyses, proportional hazard analyses, and a multivariate Cox regression analysis.
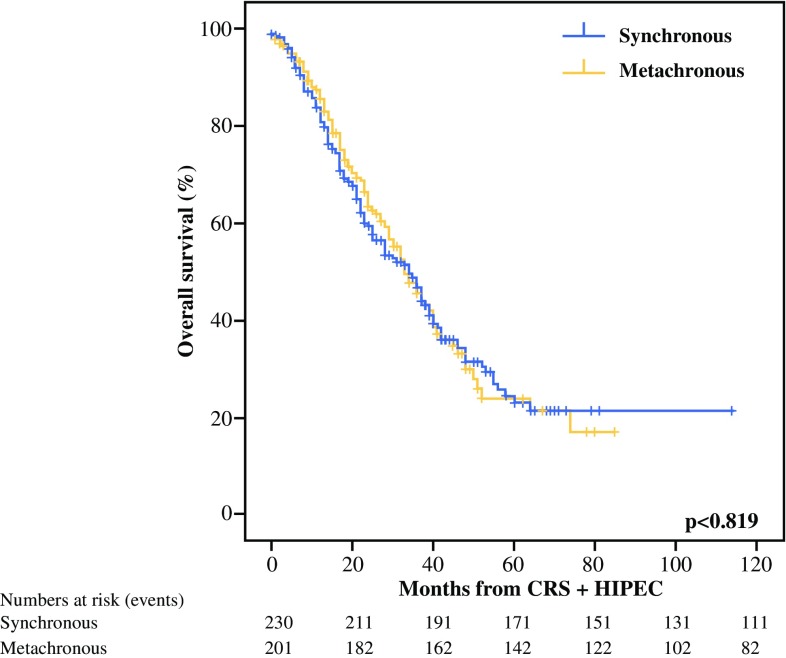
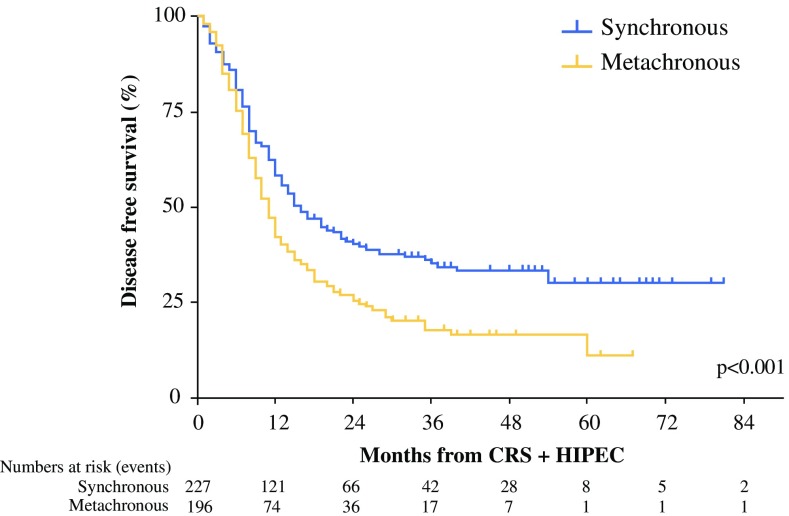
The study enrolled 433 patients, of whom 231 (53%) had synchronous colorectal PM and 202 (47%) had metachronous colorectal PM. The major postoperative complication rate and median OS were similar between the patients with synchronous colorectal PM and those with metachronous colorectal PM (26.8% vs 29.7%; p = 0.693 and 34 vs 33 months, respectively; p = 0.819). The median DFS was significantly decreased for the patients with metachronous colorectal PM and those with synchronous colorectal PM (11 vs 15 months; adjusted hazard ratio, 1.63; 95% confidence interval, 1.18-2.26).
Metachronous onset of colorectal PM is associated with early recurrence after CRS with HIPEC compared with synchronous colorectal PM, without a difference in OS or major postoperative complications. Time to onset of colorectal PM should be taken into consideration to optimize patient selection for this major procedure.
仔细选择接受结直肠腹膜转移(PM)细胞减灭术(CRS)联合腹腔热灌注化疗(HIPEC)的患者至关重要。目前尚不清楚结直肠 PM 的发病时间(同步或异时)是否会影响 CRS 联合 HIPEC 后的手术发病率和生存结局。
从两个荷兰三级转诊医院的一个前瞻性维护数据库中回顾性纳入 2006 年 2 月至 2017 年 12 月期间接受 CRS 联合 HIPEC 治疗的组织学证实的结直肠 PM 患者。将结直肠 PM 的发病时间分为同步(在结直肠癌初始表现时诊断为 PM)或异时(在初始结直肠切除术治愈后诊断为 PM)。使用 Kaplan-Meier 分析、比例风险分析和多变量 Cox 回归分析比较同步结直肠 PM 患者和异时结直肠 PM 患者之间的主要术后并发症(Clavien-Dindo 分级≥3)、总生存期(OS)和无病生存期(DFS)。
该研究纳入了 433 名患者,其中 231 名(53%)患者为同步结直肠 PM,202 名(47%)患者为异时结直肠 PM。同步结直肠 PM 患者和异时结直肠 PM 患者的主要术后并发症发生率和中位 OS 相似(26.8%比 29.7%;p=0.693 和 34 比 33 个月,分别;p=0.819)。异时结直肠 PM 患者和同步结直肠 PM 患者的中位 DFS 显著降低(11 比 15 个月;调整后的危险比,1.63;95%置信区间,1.18-2.26)。
与同步结直肠 PM 相比,异时结直肠 PM 的发病时间与 CRS 联合 HIPEC 后的早期复发相关,而 OS 或主要术后并发症无差异。结直肠 PM 的发病时间应考虑在内,以优化该主要手术的患者选择。