Rocky Mountain Poison & Drug Center, Denver Health and Hospital Authority, Denver, Colorado.
Janssen Pharmaceutical Research & Development LLC, Titusville, New Jersey.
Pain Med. 2020 Jan 1;21(1):92-100. doi: 10.1093/pm/pnz031.
To assess changes in mortality rates in extended-release and long-acting (ER/LA) opioid analgesics after the implementation of the Risk Evaluation and Mitigation Strategy (REMS).
All drug poisoning deaths in three states: Florida, Oregon, and Washington. Data were obtained through state vital records offices and the Researched Abuse, Diversion and Addiction-Related Surveillance System Medical Examiner Program.
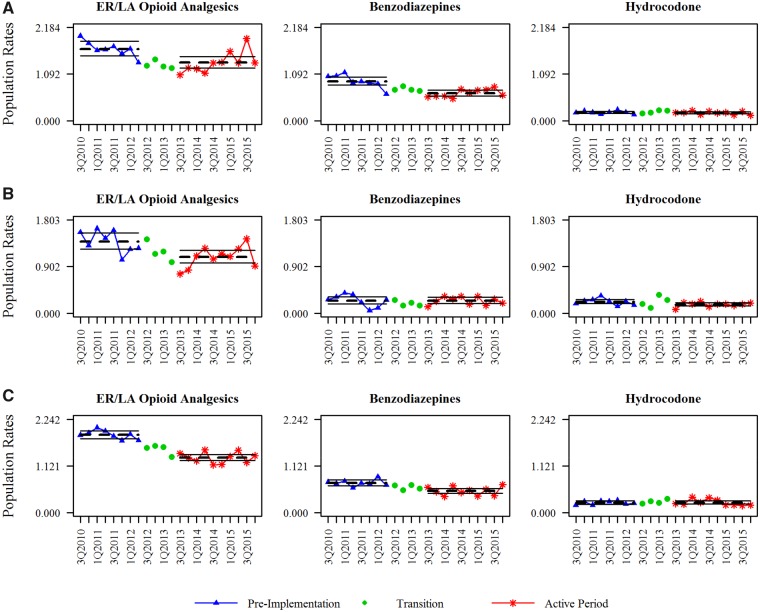
Using cause-of-death literal text from death certificates, individual opioid active pharmaceutical ingredients (APIs) involved in each death were identified using rules-based natural language processing. Population-adjusted and prescriptions dispensed-adjusted mortality rates were calculated for all ER/LA opioid analgesic and individual opioid APIs. Rates before and after implementation of the REMS were compared. Rate changes were compared with rates from two APIs with little or no inclusion in the REMS: benzodiazepines and hydrocodone.
The mean ER/LA opioid analgesic population-adjusted mortality rate significantly decreased in all three states (FL: P = 0.003; OR: P = 0.003; WA: P < 0.001). Mortality rates for benzodiazepines and hydrocodone also decreased and were not statistically different. Significant heterogeneity in mortality rates of individual opioids was observed between the three states. When adjusted for prescription volume, the ER/LA opioid analgesic mortality rate decreased in all three states, but was significant only for Washington (P < 0.001).
The population-adjusted mortality rate of ER/LA opioid analgesics has decreased in three states. Notably, the contributions to mortality rates by individual opioid analgesics were not uniform across the three states in this study. However, these changes were not generally distinct from changes in mortality rates where comparator substances were involved.
评估风险评估和缓解策略(REMS)实施后,延长释放和长效(ER/LA)阿片类镇痛药的死亡率变化。
三个州的所有药物中毒死亡:佛罗里达州、俄勒冈州和华盛顿州。数据通过州生命记录办公室和研究滥用、转移和成瘾相关监测系统法医计划获得。
使用死亡证明中的死因文字,使用基于规则的自然语言处理,确定涉及每个死亡的个体阿片类药物活性药物成分(API)。计算了所有 ER/LA 阿片类镇痛药和个体阿片类 API 的人群调整和处方调整死亡率。比较了 REMS 实施前后的死亡率。将变化率与 REMS 中包含较少或没有的两种 API(苯二氮䓬类药物和氢可酮)的变化率进行比较。
所有三个州的 ER/LA 阿片类镇痛药人群调整死亡率均显著降低(FL:P=0.003;OR:P=0.003;WA:P<0.001)。苯二氮䓬类药物和氢可酮的死亡率也有所下降,但无统计学差异。在三个州之间观察到个体阿片类药物死亡率的显著异质性。当调整处方量时,所有三个州的 ER/LA 阿片类镇痛药死亡率均降低,但仅在华盛顿州有统计学意义(P<0.001)。
三个州的 ER/LA 阿片类镇痛药人群调整死亡率有所下降。值得注意的是,在本研究中,个体阿片类镇痛药对死亡率的贡献在三个州之间并不均匀。然而,这些变化与涉及比较物质的死亡率变化并没有明显区别。