Iqbal Umair, Perumpail Brandon J, Akhtar Daud, Kim Donghee, Ahmed Aijaz
Department of Medicine, Geisinger Commonwealth School of Medicine, Danville, PA 17822, USA.
Department of Medicine, Drexel University College of Medicine, Philadelphia, PA 19129, USA.
Medicines (Basel). 2019 Mar 18;6(1):41. doi: 10.3390/medicines6010041.
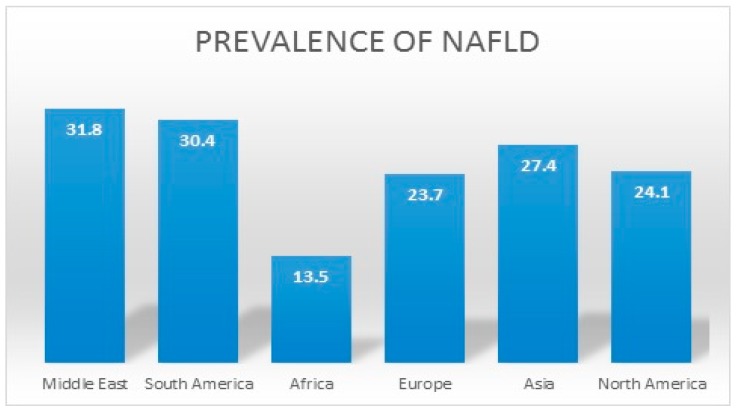
Nonalcoholic fatty liver disease (NAFLD) encompasses a wide spectrum of liver damage from the more prevalent (75%⁻80%) and nonprogressive nonalcoholic fatty liver (NAFL) category to its less common and more ominous subset, nonalcoholic steatohepatitis (NASH). NAFLD is now the most common cause of chronic liver disease in the developed world and is a leading indication for liver transplantation in United States (US). The global prevalence of NAFLD is estimated to be 25%, with the lowest prevalence in Africa (13.5%) and highest in the Middle East (31.8%) and South America (30.4%). The increasing incidence of NAFLD has been associated with the global obesity epidemic and manifestation of metabolic complications, including hypertension, diabetes, and dyslipidemia. The rapidly rising healthcare and economic burdens of NAFLD warrant institution of preventative and treatment measures in the high-risk sub-populations in an effort to reduce the morbidity and mortality associated with NAFLD. Genetic, demographic, clinical, and environmental factors may play a role in the pathogenesis of NAFLD. While NAFLD has been linked with various genetic variants, including PNPLA-3, TM6SF2, and FDFT1, environmental factors may predispose individuals to NAFLD as well. NAFLD is more common in older age groups and in men. With regards to ethnicity, in the US, Hispanics have the highest prevalence of NAFLD, followed by Caucasians and then African-Americans. NAFLD is frequently associated with the components of metabolic syndrome, such as type 2 diabetes mellitus (T2DM), obesity, hypertension, and dyslipidemia. Several studies have shown that the adoption of a healthy lifestyle, weight loss, and pro-active management of individual components of metabolic syndrome can help to prevent, retard or reverse NAFLD-related liver damage. Independently, NAFLD increases the risk of premature cardiovascular disease and associated mortality. For this reason, a case can be made for screening of NAFLD to facilitate early diagnosis and to prevent the hepatic and extra-hepatic complications in high risk sub-populations with morbid obesity, diabetes, and other metabolic risk factors.
非酒精性脂肪性肝病(NAFLD)涵盖了广泛的肝脏损伤范围,从较为常见(75%⁻80%)且病情无进展的非酒精性脂肪肝(NAFL)类别,到其较不常见且更为严重的子集——非酒精性脂肪性肝炎(NASH)。NAFLD现已成为发达国家慢性肝病的最常见病因,并且是美国肝脏移植的主要指征。据估计,NAFLD在全球的患病率为25%,其中非洲患病率最低(13.5%),中东(31.8%)和南美洲(30.4%)患病率最高。NAFLD发病率的不断上升与全球肥胖流行以及代谢并发症的出现有关,这些并发症包括高血压、糖尿病和血脂异常。NAFLD迅速增加的医疗保健和经济负担促使在高危亚人群中采取预防和治疗措施,以努力降低与NAFLD相关的发病率和死亡率。遗传、人口统计学、临床和环境因素可能在NAFLD的发病机制中起作用。虽然NAFLD与多种基因变异有关,包括PNPLA - 3、TM6SF2和FDFT1,但环境因素也可能使个体易患NAFLD。NAFLD在老年人群和男性中更为常见。就种族而言,在美国,西班牙裔NAFLD患病率最高,其次是白种人,然后是非洲裔美国人。NAFLD常与代谢综合征的组成部分相关,如2型糖尿病(T2DM)、肥胖、高血压和血脂异常。多项研究表明,采取健康的生活方式、减轻体重以及积极管理代谢综合征的各个组成部分有助于预防、延缓或逆转与NAFLD相关的肝脏损伤。此外,NAFLD会增加过早发生心血管疾病及相关死亡率的风险。因此,有理由对NAFLD进行筛查,以便在患有病态肥胖、糖尿病和其他代谢危险因素的高危亚人群中促进早期诊断并预防肝脏和肝外并发症。