Huh Youn, Cho Yoon Jeong, Nam Ga Eun
Department of Family Medicine, Uijeongbu Eulji Medical Center, Eulji University School of Medicine, Uijeongbu, Korea.
Department of Family Medicine, Daegu Catholic University School of Medicine, Daegu, Korea.
J Obes Metab Syndr. 2022 Mar 30;31(1):17-27. doi: 10.7570/jomes22021.
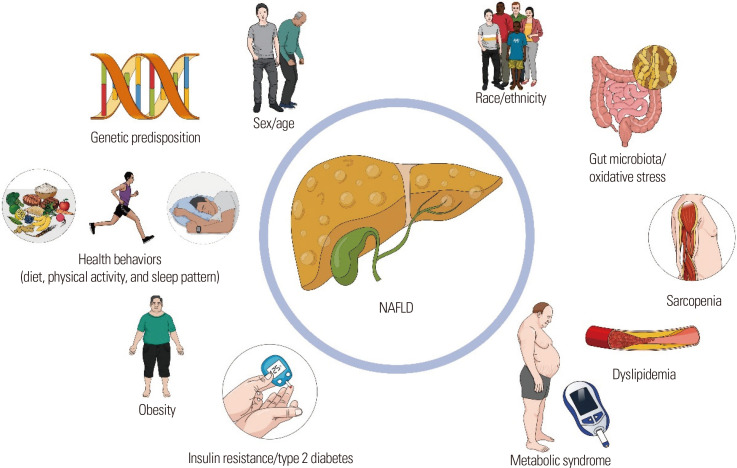
Because of the global obesity epidemic, the incidence and prevalence of nonalcoholic fatty liver disease (NAFLD) have increased worldwide, including among Koreans. Recently, the incidence rate of NAFLD in Korea was reported to be 45.1 per 1,000 person-years, and the prevalence as approximately 30% depending on the diagnostic methods used. The incidence of advanced fibrosis and hepatocellular carcinoma, as well as all-cause and liver-related mortality in NAFLD patients has increased substantially, imposing considerable public health costs in Korea. Genetic, demographic, environmental, and clinical factors are involved in the pathogenesis of NAFLD. Some genetic variants, such as patatin-like phospholipase domain-containing 3 () and sorting and assembly machinery component 50 (), play a major role in the occurrence of NAFLD. The risk of NAFLD and fibrosis increases with advancing age and in men. Nutritional factors, inadequate exercise, and sleep duration are also associated with increased risk of NAFLD. Obesity is a major risk factor for NAFLD; however, NAFLD in lean individuals has been noted in recent studies. Insulin resistance, type 2 diabetes, and metabolic syndrome and its components are closely associated with NAFLD development and liver fibrosis with various underlying mechanisms. Sarcopenia likely shares a common pathophysiology with NAFLD. The rapidly increasing incidence and prevalence of NAFLD and its complications, as well as the associated healthcare burden, warrant early assessment of NAFLD and its risk factors to prevent NAFLD-related complications in high risk groups.
由于全球肥胖流行,非酒精性脂肪性肝病(NAFLD)的发病率和患病率在全球范围内都有所上升,包括韩国人。最近,据报道韩国NAFLD的发病率为每1000人年45.1例,根据所使用的诊断方法,患病率约为30%。NAFLD患者中晚期纤维化和肝细胞癌的发病率以及全因死亡率和肝脏相关死亡率大幅上升,给韩国带来了相当大的公共卫生成本。遗传、人口统计学、环境和临床因素都参与了NAFLD的发病机制。一些基因变异,如含patatin样磷脂酶结构域3()和分选与组装机制组件50(),在NAFLD的发生中起主要作用。NAFLD和纤维化的风险随着年龄增长和男性而增加。营养因素、运动不足和睡眠时间也与NAFLD风险增加有关。肥胖是NAFLD的主要危险因素;然而,最近的研究中也注意到瘦人患NAFLD的情况。胰岛素抵抗、2型糖尿病、代谢综合征及其组成部分与NAFLD的发展和肝纤维化密切相关,其潜在机制各不相同。肌肉减少症可能与NAFLD有共同的病理生理学。NAFLD及其并发症的发病率和患病率迅速上升,以及相关的医疗负担,需要对NAFLD及其危险因素进行早期评估,以预防高危人群中与NAFLD相关的并发症。