Medical Image Computing, University of Bremen, Bremen, Germany; Fraunhofer MEVIS, Bremen, Germany; Surgical Planning Laboratory, Brigham and Women's Hospital, Harvard Medical School, Boston, USA.
Fraunhofer MEVIS, Bremen, Germany.
Neuroimage Clin. 2019;22:101766. doi: 10.1016/j.nicl.2019.101766. Epub 2019 Mar 12.
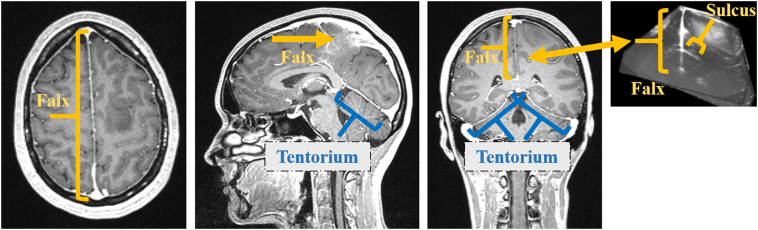
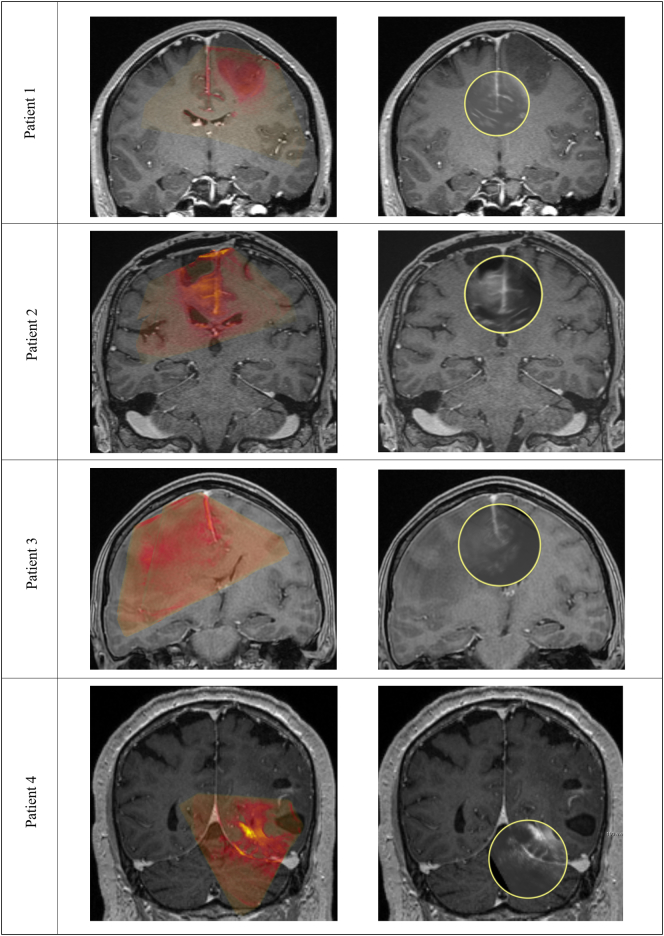
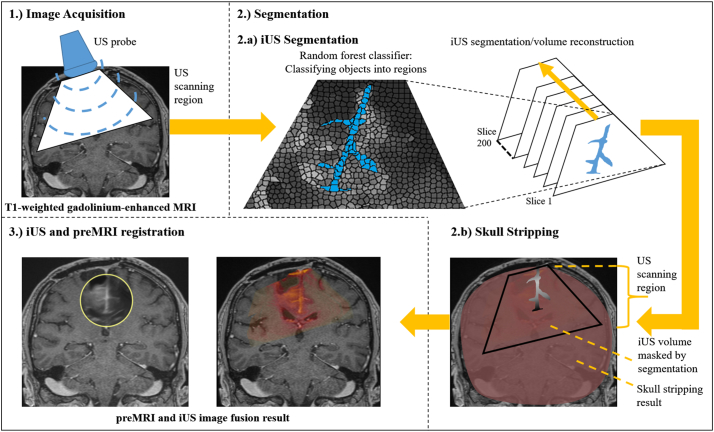
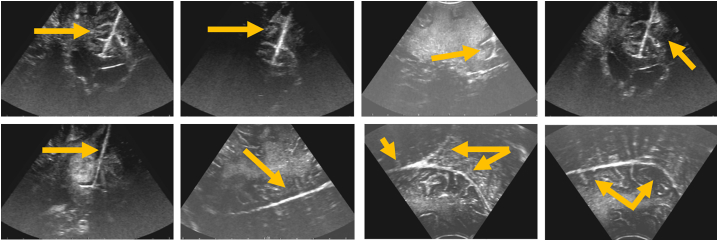
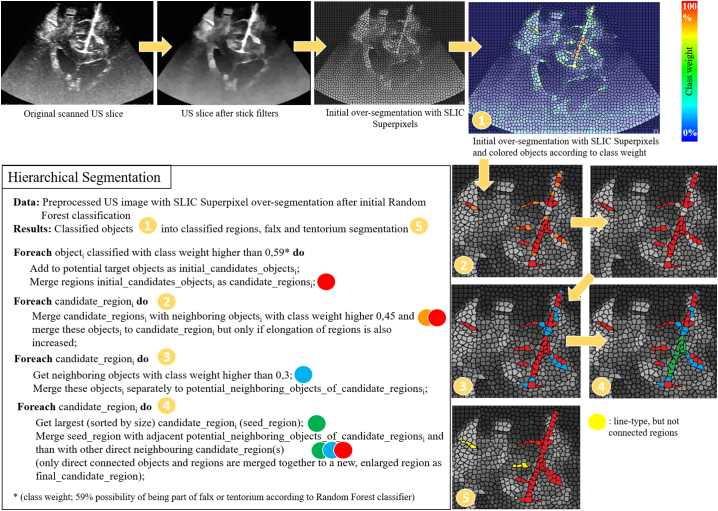
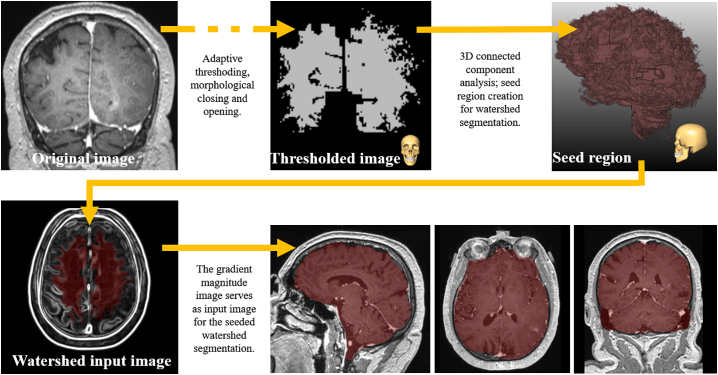
Knowledge of the exact tumor location and structures at risk in its vicinity are crucial for neurosurgical interventions. Neuronavigation systems support navigation within the patient's brain, based on preoperative MRI (preMRI). However, increasing tissue deformation during the course of tumor resection reduces navigation accuracy based on preMRI. Intraoperative ultrasound (iUS) is therefore used as real-time intraoperative imaging. Registration of preMRI and iUS remains a challenge due to different or varying contrasts in iUS and preMRI. Here, we present an automatic and efficient segmentation of B-mode US images to support the registration process. The falx cerebri and the tentorium cerebelli were identified as examples for central cerebral structures and their segmentations can serve as guiding frame for multi-modal image registration. Segmentations of the falx and tentorium were performed with an average Dice coefficient of 0.74 and an average Hausdorff distance of 12.2 mm. The subsequent registration incorporates these segmentations and increases accuracy, robustness and speed of the overall registration process compared to purely intensity-based registration. For validation an expert manually located corresponding landmarks. Our approach reduces the initial mean Target Registration Error from 16.9 mm to 3.8 mm using our intensity-based registration and to 2.2 mm with our combined segmentation and registration approach. The intensity-based registration reduced the maximum initial TRE from 19.4 mm to 5.6 mm, with the approach incorporating segmentations this is reduced to 3.0 mm. Mean volumetric intensity-based registration of preMRI and iUS took 40.5 s, including segmentations 12.0 s.
了解肿瘤的确切位置及其附近的危险结构对于神经外科手术至关重要。神经导航系统基于术前 MRI(preMRI)支持在患者大脑内进行导航。然而,在肿瘤切除过程中,组织变形的增加会降低基于 preMRI 的导航准确性。因此,术中超声(iUS)被用作实时术中成像。由于 iUS 和 preMRI 之间存在不同或变化的对比度,因此 preMRI 和 iUS 的配准仍然是一个挑战。在这里,我们提出了一种自动且高效的 B 型 US 图像分割方法,以支持配准过程。大脑镰和小脑幕作为中央脑结构的示例被识别出来,其分割可以作为多模态图像配准的指导框架。大脑镰和小脑幕的分割平均 Dice 系数为 0.74,平均 Hausdorff 距离为 12.2mm。随后的配准结合了这些分割,与纯基于强度的配准相比,提高了整体配准过程的准确性、鲁棒性和速度。为了验证,一位专家手动定位了相应的地标。我们的方法使用基于强度的配准将初始平均目标配准误差从 16.9mm 降低到 3.8mm,使用我们的组合分割和配准方法将其降低到 2.2mm。基于强度的配准将初始最大 TRE 从 19.4mm 降低到 5.6mm,采用包含分割的方法,将其降低到 3.0mm。preMRI 和 iUS 的基于强度的平均配准耗时 40.5 秒,包括分割耗时 12.0 秒。