Saß Benjamin, Zivkovic Darko, Pojskic Mirza, Nimsky Christopher, Bopp Miriam H A
Department of Neurosurgery, University of Marburg, Marburg, Germany.
Center for Mind, Brain and Behavior (CMBB), Marburg, Germany.
Front Neurosci. 2022 May 9;16:883584. doi: 10.3389/fnins.2022.883584. eCollection 2022.
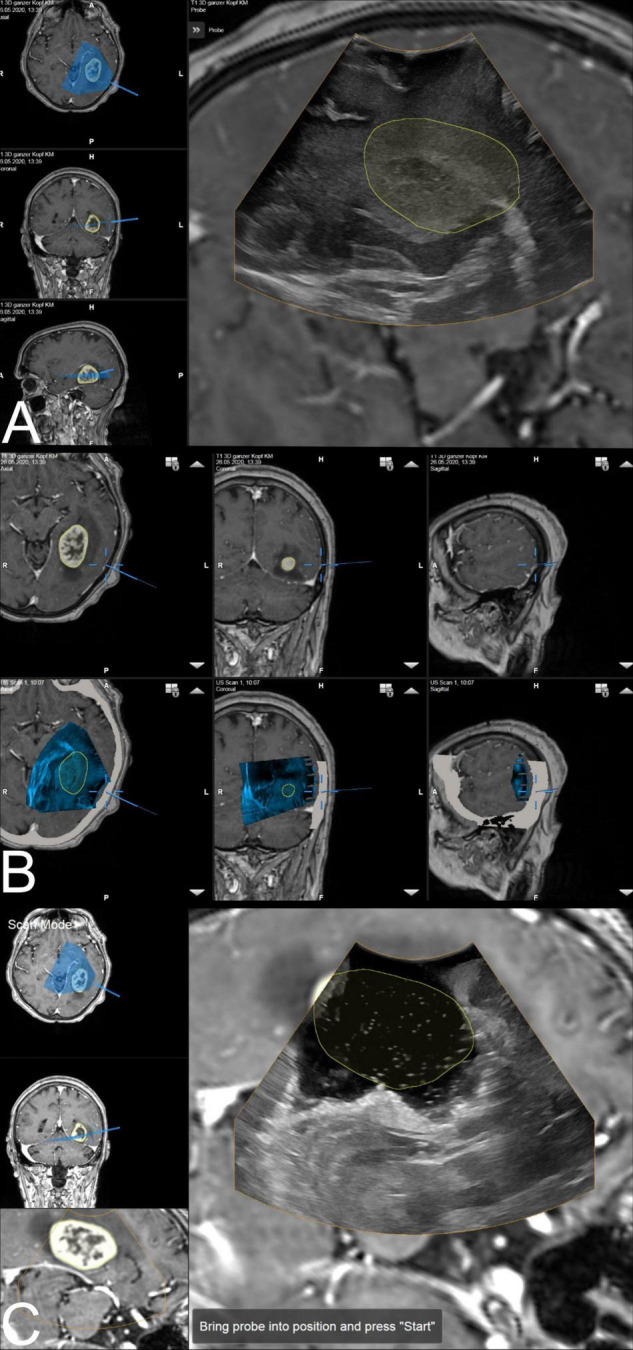
Neuronavigation is routinely used in glioblastoma surgery, but its accuracy decreases during the operative procedure due to brain shift, which can be addressed utilizing intraoperative imaging. Intraoperative ultrasound (iUS) is widely available, offers excellent live imaging, and can be fully integrated into modern navigational systems. Here, we analyze the imaging features of navigated i3D US and its impact on the extent of resection (EOR) in glioblastoma surgery.
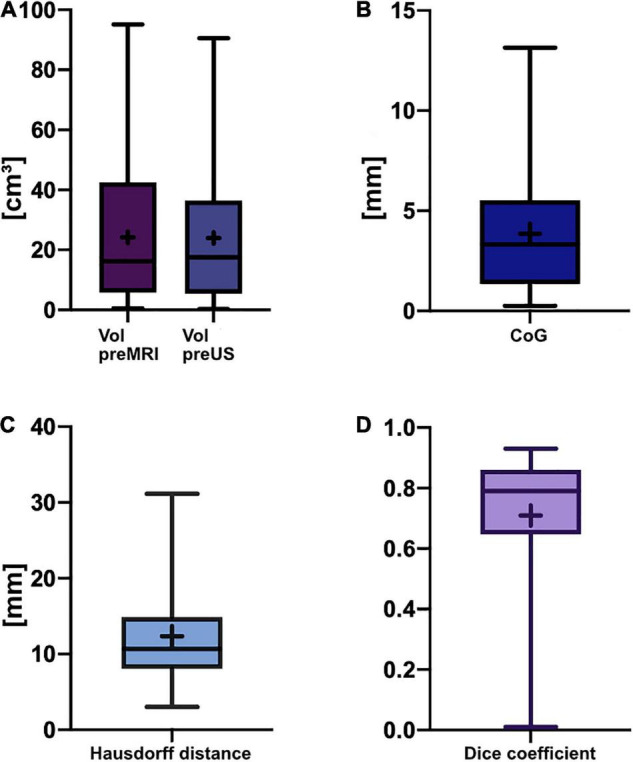
Datasets of 31 glioblastoma resection procedures were evaluated. Patient registration was established using intraoperative computed tomography (iCT). Pre-operative MRI (pre-MRI) and pre-resectional ultrasound (pre-US) datasets were compared regarding segmented tumor volume, spatial overlap (Dice coefficient), the Euclidean distance of the geometric center of gravity (CoG), and the Hausdorff distance. Post-resectional ultrasound (post-US) and post-operative MRI (post-MRI) tumor volumes were analyzed and categorized into subtotal resection (STR) or gross total resection (GTR) cases.
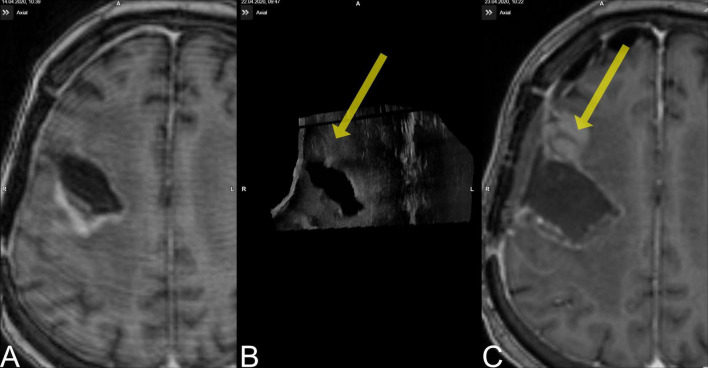
The mean patient age was 59.3 ± 11.9 years. There was no significant difference in pre-resectional segmented tumor volumes (pre-MRI: 24.2 ± 22.3 cm; pre-US: 24.0 ± 21.8 cm). The Dice coefficient was 0.71 ± 0.21, the Euclidean distance of the CoG was 3.9 ± 3.0 mm, and the Hausdorff distance was 12.2 ± 6.9 mm. A total of 18 cases were categorized as GTR, 10 cases were concordantly classified as STR on MRI and ultrasound, and 3 cases had to be excluded from post-resectional analysis. In four cases, i3D US triggered further resection.
Navigated i3D US is reliably adjunct in a multimodal navigational setup for glioblastoma resection. Tumor segmentations revealed similar results in i3D US and MRI, demonstrating the capability of i3D US to delineate tumor boundaries. Additionally, i3D US has a positive influence on the EOR, allows live imaging, and depicts brain shift.
神经导航在胶质母细胞瘤手术中常规使用,但由于脑移位,其准确性在手术过程中会降低,可通过术中成像来解决。术中超声(iUS)广泛可用,提供出色的实时成像,并且可以完全集成到现代导航系统中。在此,我们分析导航i3D US 的成像特征及其对胶质母细胞瘤手术中切除范围(EOR)的影响。
评估了31例胶质母细胞瘤切除手术的数据集。使用术中计算机断层扫描(iCT)进行患者配准。比较术前MRI(pre-MRI)和切除前超声(pre-US)数据集的分割肿瘤体积、空间重叠(Dice系数)、几何重心(CoG)的欧几里得距离和豪斯多夫距离。分析切除后超声(post-US)和术后MRI(post-MRI)肿瘤体积,并将其分类为次全切除(STR)或全切除(GTR)病例。
患者平均年龄为59.3±11.9岁。切除前分割肿瘤体积无显著差异(pre-MRI:24.2±22.3 cm;pre-US:24.0±21.8 cm)。Dice系数为0.71±0.21,CoG的欧几里得距离为3.9±3.0 mm,豪斯多夫距离为12.2±6.9 mm。共有18例被分类为GTR,10例在MRI和超声上均一致分类为STR,3例必须排除在切除后分析之外。在4例中,i3D US触发了进一步切除。
导航i3D US在胶质母细胞瘤切除的多模态导航设置中是可靠的辅助手段。肿瘤分割在i3D US和MRI中显示出相似的结果,证明了i3D US描绘肿瘤边界的能力。此外,i3D US对EOR有积极影响,允许实时成像,并描绘脑移位。