Faculty of Health Sciences, University of Hull, Kingston upon Hull, HU6 7RX, UK.
Hull York Medical School, University of Hull, Kingston upon Hull, HU6 7RX, UK.
BMC Cancer. 2019 Mar 22;19(1):259. doi: 10.1186/s12885-019-5465-z.
Though the management of malignancies has improved vastly in recent years, many treatment options lack the desired efficacy and fail to adequately augment patient morbidity and mortality. It is increasingly clear that patient response to therapy is unique to each individual, necessitating personalised, or 'precision' medical care. This demand extends to thyroid cancer; ~ 10% patients fail to respond to radioiodine treatment due to loss of phenotypic differentiation, exposing the patient to unnecessary ionising radiation, as well as delaying treatment with alternative therapies.
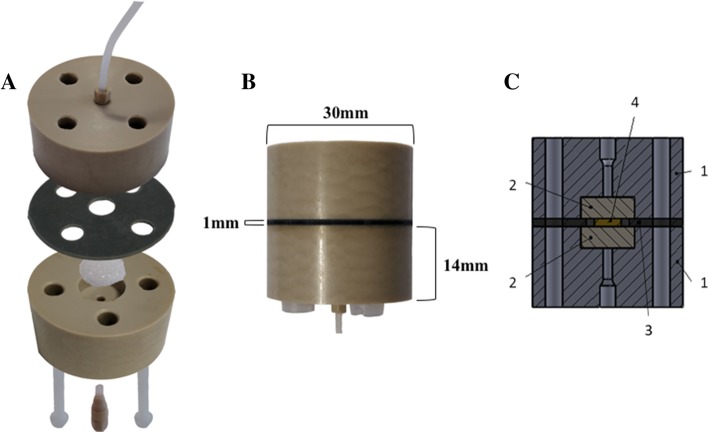
Human thyroid tissue (n = 23, malignant and benign) was live-sliced (5 mm diameter × 350-500 μm thickness) then analysed or incorporated into a microfluidic culture device for 96 h (37 °C). Successful maintenance of tissue was verified by histological (H&E), flow cytometric propidium iodide or trypan blue uptake, immunohistochemical (Ki67 detection/ BrdU incorporation) and functional analysis (thyroxine [T4] output) in addition to analysis of culture effluent for the cell death markers lactate dehydrogenase (LDH) and dead-cell protease (DCP). Apoptosis was investigated by Terminal deoxynucleotidyl transferase dUTP nick end labelling (TUNEL). Differentiation was assessed by evaluation of thyroid transcription factor (TTF1) and sodium iodide symporter (NIS) expression (western blotting).
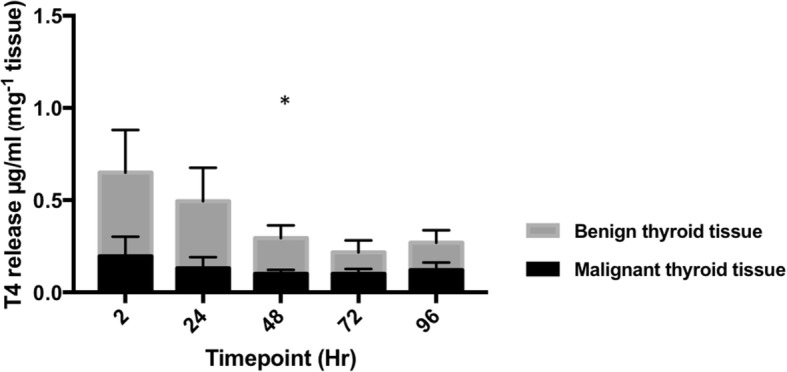
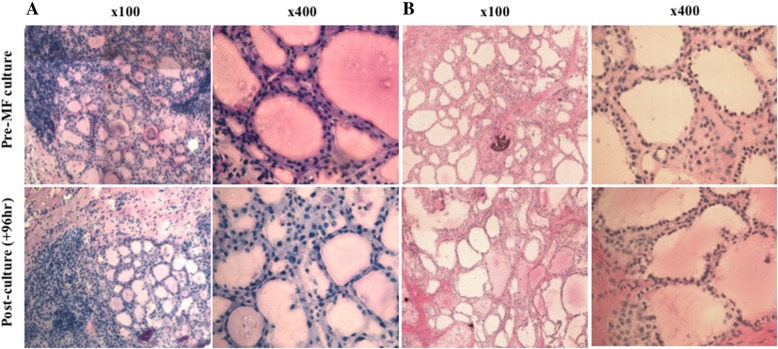
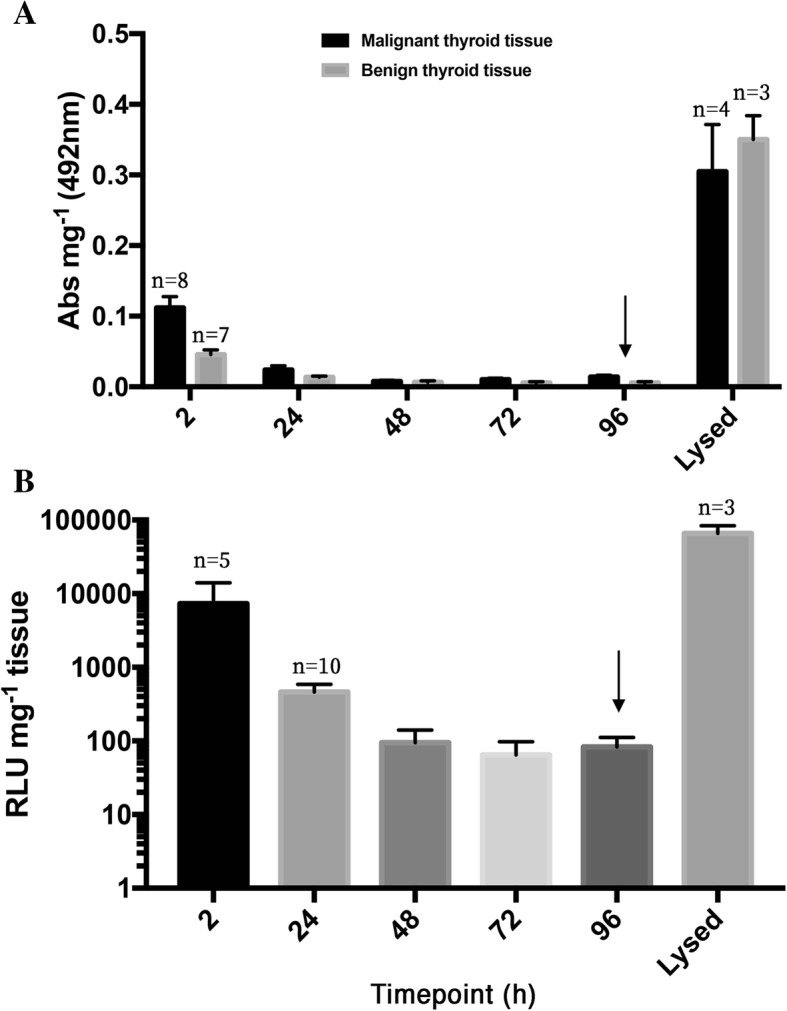
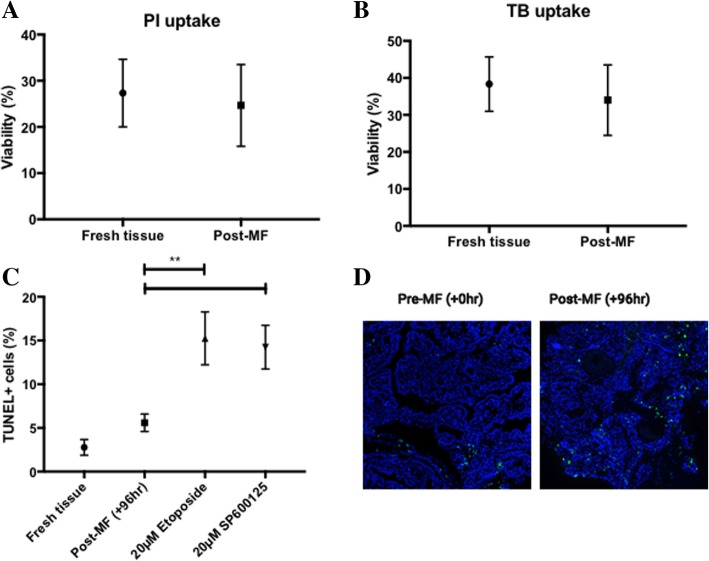
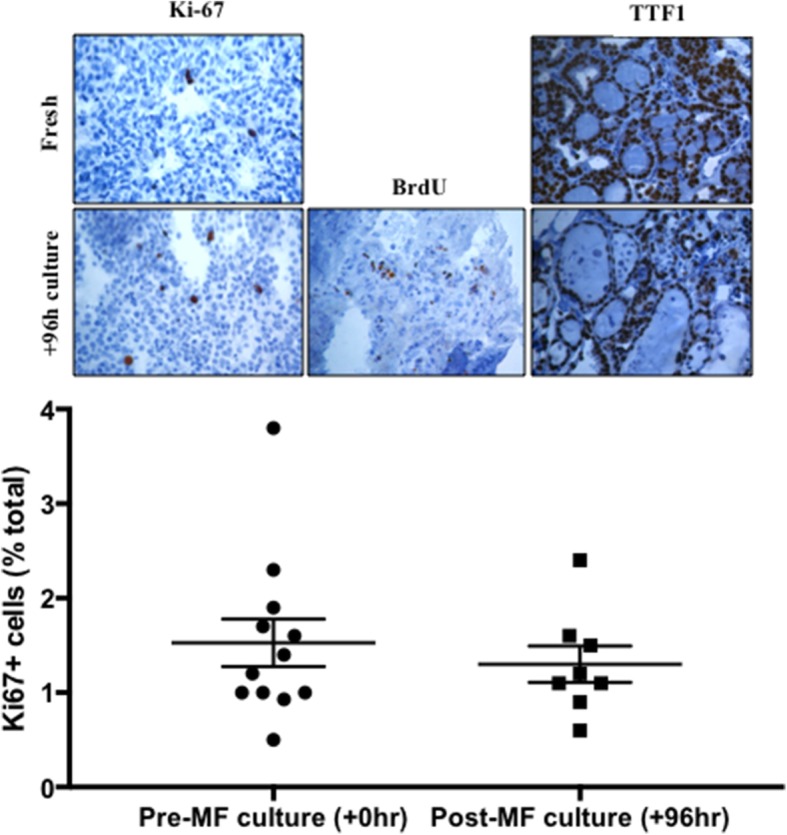
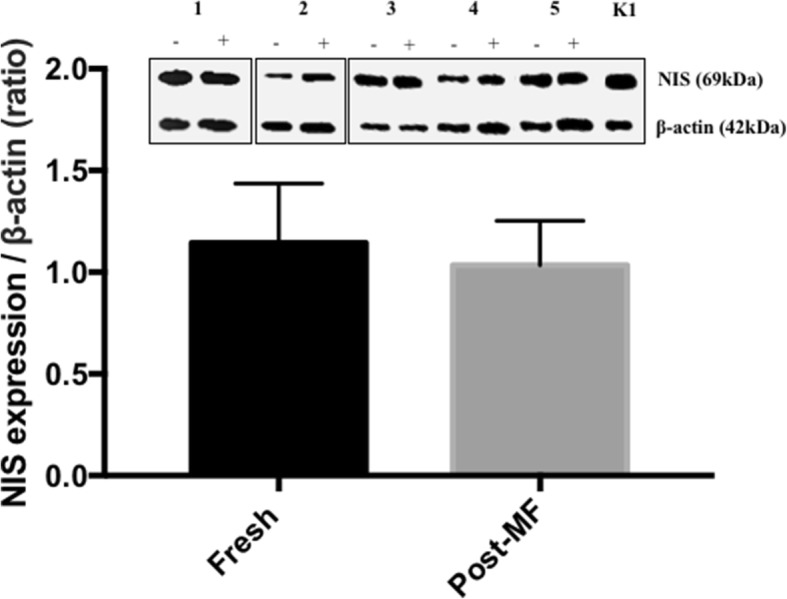
Maintenance of gross tissue architecture was observed. Analysis of dissociated primary thyroid cells using flow cytometry both prior to and post culture demonstrated no significant change in the proportion of viable cells. LDH and DCP release from on-chip thyroid tissue indicated that after an initial raised level of release, signifying cellular damage, detectable levels dropped markedly. A significant increase in apoptosis (p < 0.01) was observed after tissue was perfused with etoposide and JNK inhibitor, but not in control tissue incubated for the same time period. No significant difference in Ki-67 positivity or TTF1/NIS expression was detected between fresh and post-culture thyroid tissue samples, moreover BrdU positive nuclei indicated on-chip cellular proliferation. Cultured thyroid explants were functionally viable as determined by production of T4 throughout the culture period.
The described microfluidic platform can maintain the viability of thyroid tissue slices ex vivo for a minimum of four days, providing a platform for the assessment of thyroid tissue radioiodine sensitivity/adjuvant therapies in real time.
尽管近年来恶性肿瘤的治疗有了很大的改善,但许多治疗方案的疗效并不理想,无法充分降低患者的发病率和死亡率。越来越明显的是,患者对治疗的反应因人而异,因此需要个性化或“精准”的医疗护理。这种需求也延伸到了甲状腺癌;由于表型分化丧失,约有 10%的患者对放射性碘治疗无反应,使患者暴露于不必要的电离辐射下,并延迟了替代疗法的治疗。
对 23 个人类甲状腺组织(良性和恶性)进行活体切片(直径 5 毫米×350-500 微米厚),然后进行分析或纳入微流控培养装置中培养 96 小时(37°C)。通过组织学(H&E)、碘化丙啶或台盼蓝摄取的流式细胞术、免疫组织化学(Ki67 检测/ BrdU 掺入)以及培养物渗出液中细胞死亡标志物乳酸脱氢酶(LDH)和凋亡蛋白酶(DCP)的分析来验证组织的成功维持。通过末端脱氧核苷酸转移酶 dUTP 缺口末端标记法(TUNEL)研究细胞凋亡。通过评估甲状腺转录因子(TTF1)和钠碘转运体(NIS)的表达(western blot)来评估分化。
观察到大体组织结构的维持。在培养前后使用流式细胞术对分离的原代甲状腺细胞进行分析,发现存活细胞的比例没有明显变化。来自芯片上甲状腺组织的 LDH 和 DCP 释放表明,在初始释放水平升高表示细胞损伤后,可检测到的水平明显下降。在用依托泊苷和 JNK 抑制剂灌注组织后观察到细胞凋亡显著增加(p<0.01),而在相同时间段孵育的对照组织中则没有观察到这种情况。新鲜和培养后的甲状腺组织样本之间未检测到 Ki-67 阳性率或 TTF1/NIS 表达的显著差异,此外,芯片上的 BrdU 阳性核表明细胞增殖。整个培养期间 T4 的产生证明培养的甲状腺外植体具有功能活力。
所描述的微流控平台可将甲状腺组织切片的体外活力维持至少四天,为实时评估甲状腺组织对放射性碘的敏感性/辅助治疗提供了一个平台。