Department of Environmental Health and Engineering, Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA.
Int J Epidemiol. 2019 Aug 1;48(4):1228-1239. doi: 10.1093/ije/dyz043.
Diarrhoeal outcomes in children are often ascertained using caregiver-reported symptoms, which are subject to a variety of biases and methodological challenges. One source of bias is the time window used for reporting diarrhoeal illness and the ability of caregivers to accurately recall episodes in children.
Diarrhoea period prevalence in children under five was determined using two similarly administered, nationally representative household surveys: Performance Monitoring and Accountability 2020 (PMA2020) (1-week recall, N = 14 603) and Demographic and Health Surveys (DHS) (2-week recall, N = 66 717). Countries included in the analysis were the Democratic Republic of the Congo, Ethiopia, Ghana, Kenya and Uganda. Diarrhoea period prevalence estimates were compared and water, sanitation and hygiene risk factors were analysed.
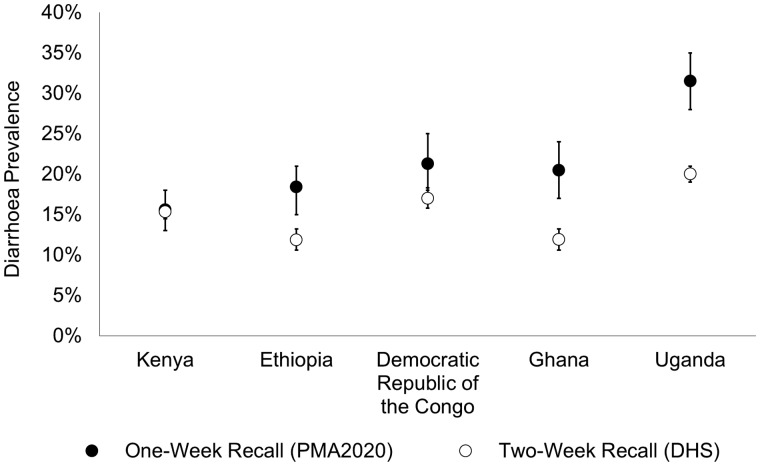
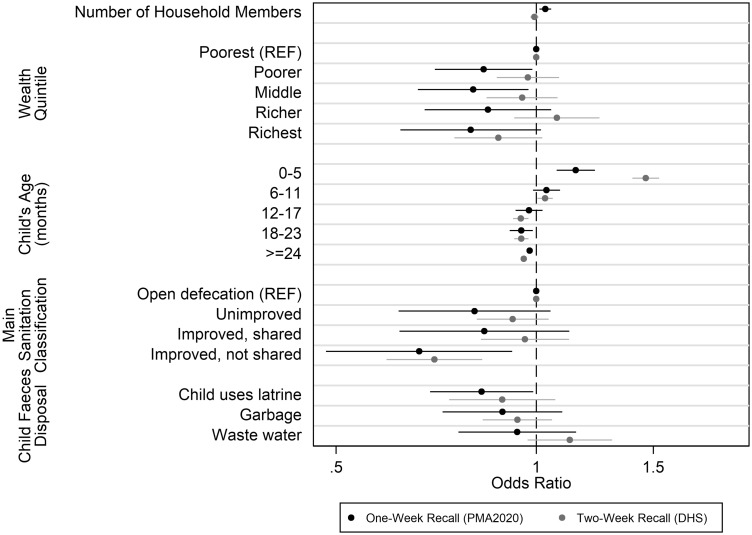
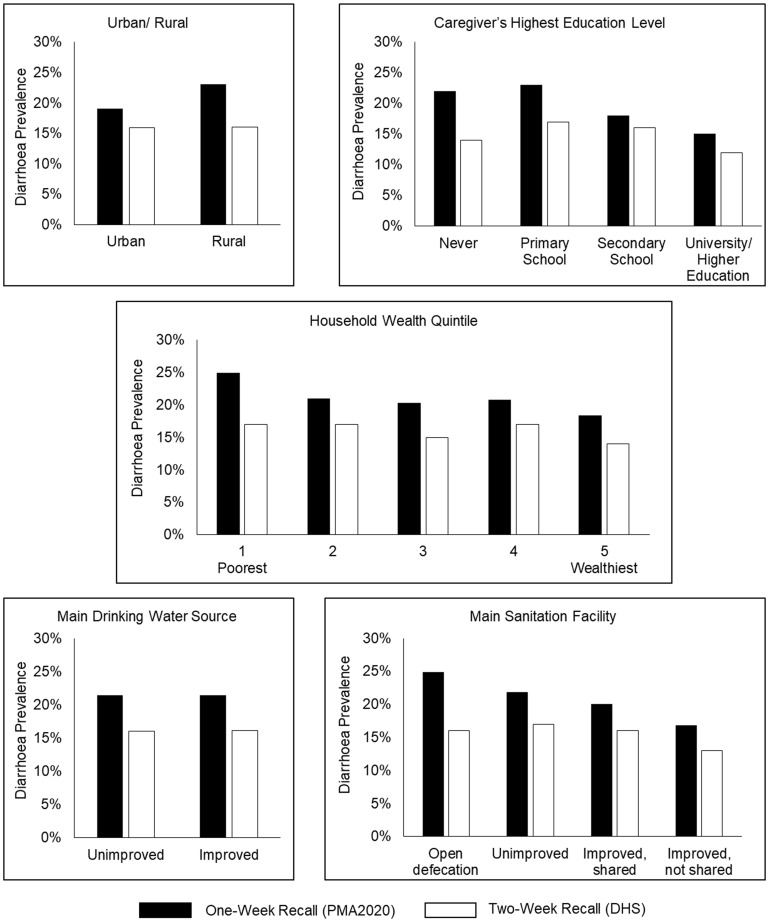
Childhood diarrhoea prevalence using 1-week recall (PMA2020) pooled across countries was 21.4% [95% confidence interval (CI): 19.9%, 22.9%] versus 16.0% using 2-week recall (DHS) (95% CI: 15.4%, 16.5%). In stratified analyses for all five countries, the number of diarrhoea cases detected was consistently higher using 1-week recall versus 2-week recall. The key risk factors identified in the PMA2020 data that were not associated with diarrhoeal episodes or were attenuated in the DHS data included: the main sanitation classifications for households, disposal method used for child faeces, number of household members and wealth quintiles.
For nationally representative household surveys assessing childhood diarrhoea period prevalence, a 2-week recall period may underestimate diarrhoea prevalence compared with a 1-week period. The household sanitation facility and practices remain key risk factors for diarrhoeal disease in children under five.
儿童腹泻结局通常通过照顾者报告的症状来确定,但这些症状受到多种偏倚和方法学挑战的影响。其中一个偏倚来源是报告腹泻病的时间窗口以及照顾者准确回忆儿童发病的能力。
使用两次类似管理的、具有全国代表性的家庭调查来确定五岁以下儿童腹泻的流行期患病率:绩效监测和问责制 2020 年调查(PMA2020)(1 周回顾,N=14603)和人口与健康调查(DHS)(2 周回顾,N=66717)。分析包括的国家有刚果民主共和国、埃塞俄比亚、加纳、肯尼亚和乌干达。比较了腹泻流行期患病率估计值,并分析了水、环境卫生和个人卫生风险因素。
在所有五个国家的分层分析中,使用 1 周回顾(PMA2020)汇总的儿童腹泻患病率为 21.4%(95%置信区间:19.9%,22.9%),而使用 2 周回顾(DHS)为 16.0%(95%置信区间:15.4%,16.5%)。在所有五个国家的分层分析中,使用 1 周回顾发现的腹泻病例数量始终高于使用 2 周回顾。在 PMA2020 数据中确定的关键风险因素与腹泻发作无关,或者在 DHS 数据中减弱,包括:家庭主要环境卫生分类、儿童粪便处理方法、家庭人口数量和财富五分位数。
对于评估儿童腹泻流行期患病率的具有全国代表性的家庭调查,与 1 周回顾期相比,2 周回顾期可能低估腹泻的患病率。家庭环境卫生设施和做法仍然是五岁以下儿童腹泻病的关键风险因素。