Huang Jing, Guo Jiquan, Li Hongtao, Huang Weibin, Zhang Tiantuo
Department of Respiratory Medicine, The Third Affiliated Hospital of Sun Yat-sen University.
Institute of Respiratory Diseases, Sun Yat-sen University.
Medicine (Baltimore). 2019 Mar;98(13):e14636. doi: 10.1097/MD.0000000000014636.
The systemic use of corticosteroids for patients in severe community-acquired pneumonia (CAP) remains disputed in clinical practice. We undertook a systematic review and meta-analysis to assess the efficacy and safety of corticosteroids in patients with severe CAP.
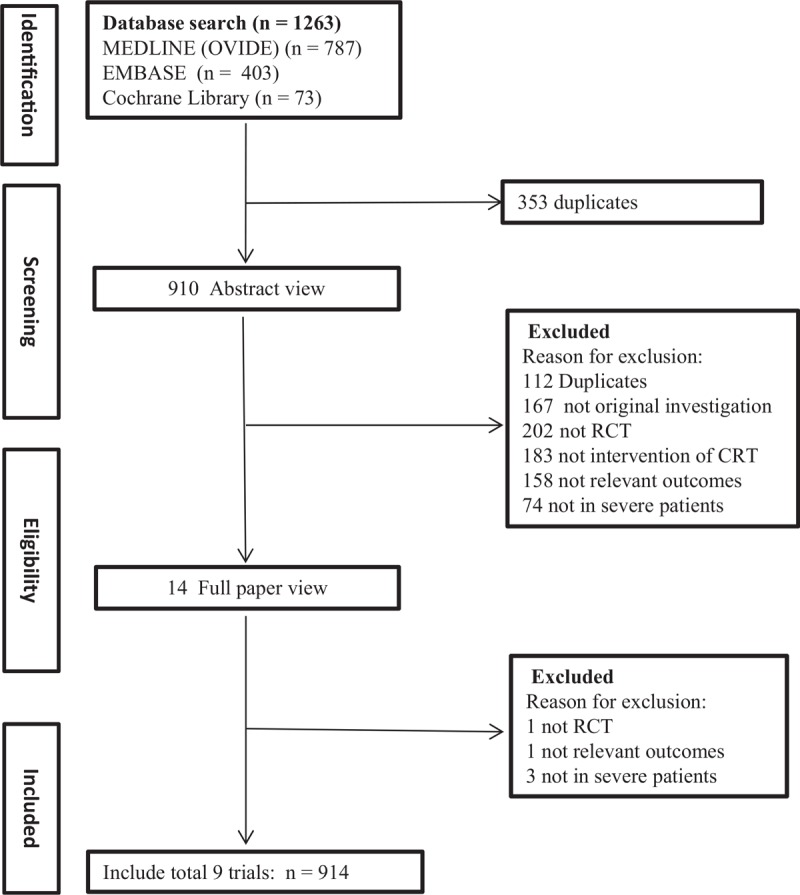
We searched MEDLINE (1946 to June 2018), EMBASE (1966 to June 2018), and the Cochrane Library database for randomized controlled trials (RCTs) conducted for severe CAP. The endpoints of the study included total mortality, length of intensive care unit (ICU) stay and mechanical ventilation.
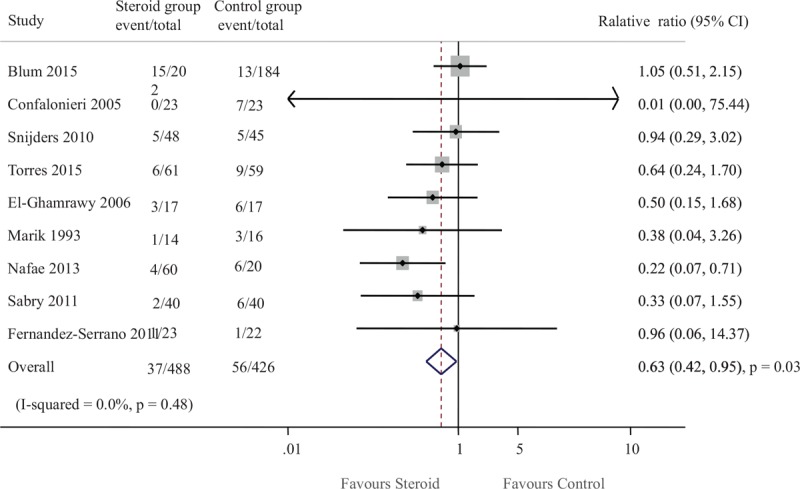
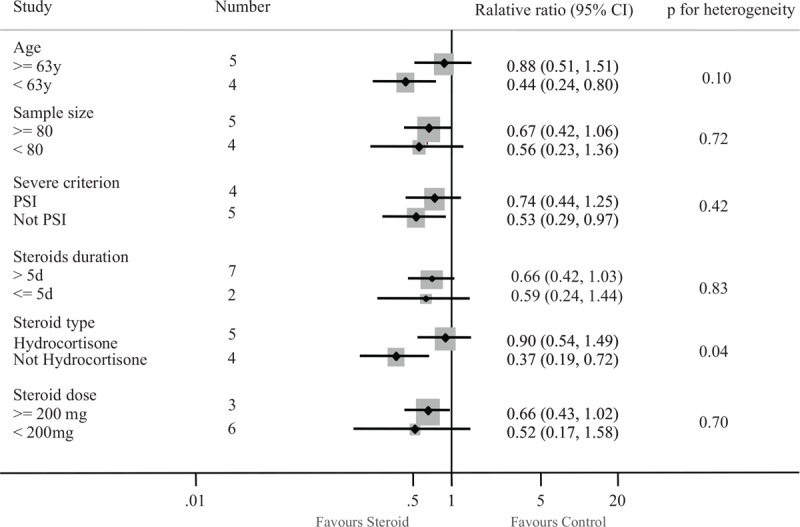
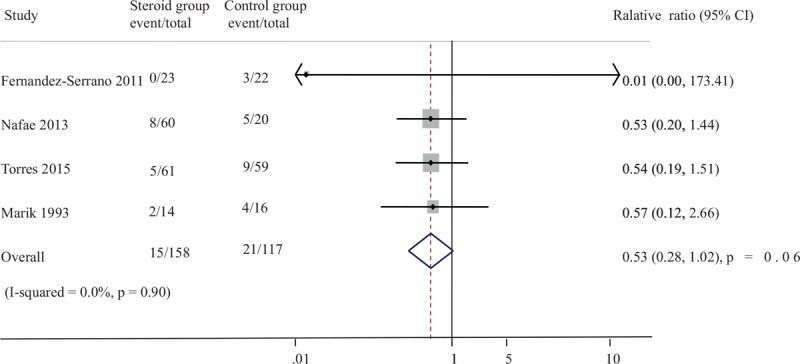
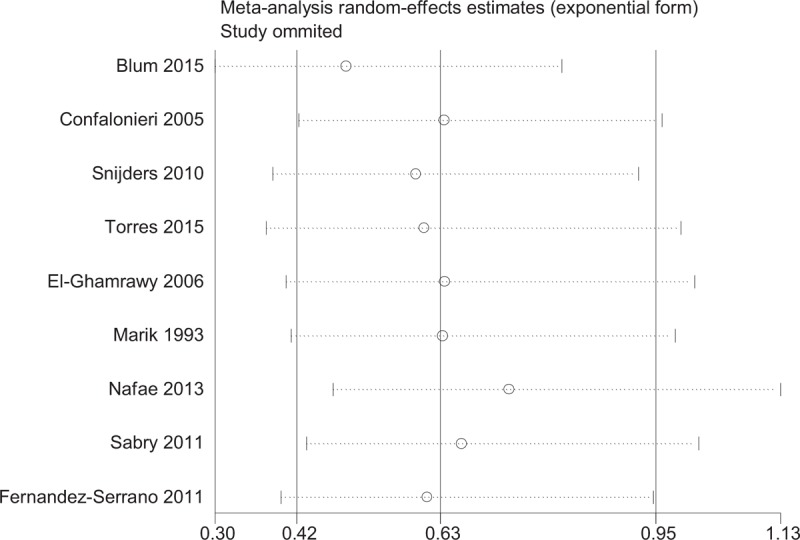
Nine trials which contained 914 patients were included for final meta-analysis. Of the 488 patients in the corticosteroid group, there were 37 deaths (7.58%) and 56 deaths occurred in 426 patients in the control group (13.1%). Corticosteroid therapy was associated with a lower rate of all-cause mortality compared to control (odd ratio [OR] 0.63, 95% confidence interval [CI] 0.42-0.95, P = .03). Subgroup analysis was conducted to show that the drug type modified the effect of steroids for mortality rate: prednisolone or methylprednisolone therapy (OR 0.37, 95% CI 0.19-0.72) reduced total mortality, whereas hydrocortisone use did not (OR 0.90, 95% CI 0.54-1.49). We found the length of ICU stay was significantly shorter in the steroid group compared to control (MD -2.52 days, 95% CI -4.88 to -0.15; P = .04). And there was a reduction trend in the need for mechanical ventilation in corticosteroid group (OR 0.53, 95% CI 0.28-1.02; P = .06). There was no trend towards more adverse events in the corticosteroid arm compared to control (OR 0.92, 95% CI 0.58-1.47; P = .74).
Overall, adjunctive systemic corticosteroids therapy was effective and safe for patients with severe CAP. In addition, the effects of mortality may differ according to the type of corticosteroids.
在临床实践中,全身使用皮质类固醇治疗重症社区获得性肺炎(CAP)患者仍存在争议。我们进行了一项系统评价和荟萃分析,以评估皮质类固醇对重症CAP患者的疗效和安全性。
我们检索了MEDLINE(1946年至2018年6月)、EMBASE(1966年至2018年6月)和Cochrane图书馆数据库,以查找针对重症CAP进行的随机对照试验(RCT)。研究终点包括总死亡率、重症监护病房(ICU)住院时间和机械通气时间。
九项试验共纳入914例患者进行最终的荟萃分析。皮质类固醇组的488例患者中有37例死亡(7.58%),对照组的426例患者中有56例死亡(13.1%)。与对照组相比,皮质类固醇治疗与全因死亡率较低相关(比值比[OR]0.63,95%置信区间[CI]0.42-0.95,P = 0.03)。亚组分析表明,药物类型改变了类固醇对死亡率的影响:泼尼松龙或甲泼尼龙治疗(OR 0.37,95% CI 0.19-0.72)降低了总死亡率,而氢化可的松则没有(OR 0.90,95% CI 0.54-1.49)。我们发现,与对照组相比,类固醇组的ICU住院时间明显更短(平均差[MD]-2.52天,95% CI -4.88至-0.15;P = 0.04)。并且皮质类固醇组机械通气需求有下降趋势(OR 0.53,95% CI 0.28-1.02;P = 0.06)。与对照组相比,皮质类固醇组没有出现更多不良事件的趋势(OR 0.92,95% CI 0.58-1.47;P = 0.74)。
总体而言,辅助全身皮质类固醇治疗对重症CAP患者有效且安全。此外,死亡率的影响可能因皮质类固醇的类型而异。