Dianet Dialysis Center, Utrecht, The Netherlands.
Department of Nephrology and Hypertension, University Medical Center Utrecht, Utrecht, The Netherlands.
BMC Nephrol. 2019 Mar 29;20(1):108. doi: 10.1186/s12882-019-1268-3.
Maximal conservative management (MCM) may be an appropriate alternative option for dialysis in some elderly patients with end-stage kidney disease (ESKD). Evidence about the impact of dialysis or MCM on quality of life (QoL) in older patients is sparse. In the GOLD (Geriatric assessment in OLder patients starting Dialysis) Study the trajectory of QoL was assessed in patients starting dialysis or MCM.
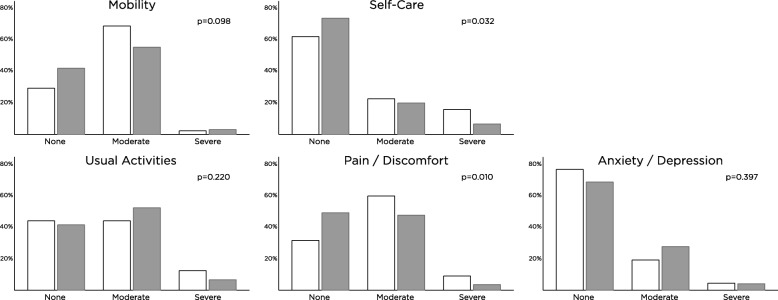
Patients ≥65 years old were included just prior to dialysis initiation or after decision for MCM. Baseline data included demographics, frailty as measured with a geriatric assessment, comorbidity (CIRS-G) and QoL, measured with the EQ-5D-3 L (EQ-5D Index and overall self-rated health). Six months follow-up data included QoL, hospitalizations and mortality. Change of QoL was assed with paired t-tests. Cox-regression was used to assess survival of MCM and dialysis patients.
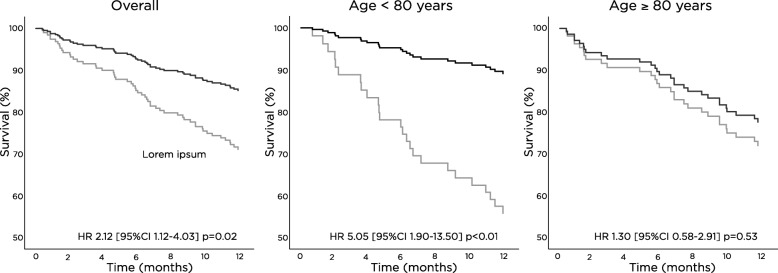
The cohort comprised 192 dialysis and 89 MCM patients. The MCM patients were older (mean age 82 ± 6 vs. 75 ± 7 years, p < 0.01) and mean kidney function was better (eGFR 11.5 ± 4.0 vs. 8.0 ± 2.9 ml/min/1.73m, p < 0.01). Baseline QoL did not differ significantly between the groups. After six months, EQ-5D Index did not improve significantly in the dialysis group with mean ± standard error (SE) 0.026 ± 0.014 (p = 0.10; not clinically relevant), but a small but clinically relevant decline was seen in the conservative group: 0.047 ± 0.022 (p < 0.01; between group difference p < 0.01). Hospitalization occurred in 50% of dialysis patients vs. 24% of conservative patients (p < 0.01). In patients over 80 years old, no survival benefit could be found for dialysis patients starting dialysis vs. MCM.
A small decline of QoL was found for conservative patients, while QoL did not change in dialysis patients. However, hospitalization rate was higher in patients starting dialysis. In patients over 80 years, no survival benefit was found.
对于终末期肾病(ESKD)的一些老年患者,最大程度的保守治疗(MCM)可能是透析的合适替代选择。关于透析或 MCM 对老年患者生活质量(QoL)影响的证据很少。在 GOLD(老年患者开始透析时的老年评估)研究中,评估了开始透析或 MCM 的患者的 QoL 轨迹。
在开始透析或决定进行 MCM 之前,纳入年龄≥65 岁的患者。基线数据包括人口统计学、老年评估测量的脆弱性、合并症(CIRS-G)和 QoL,使用 EQ-5D-3L(EQ-5D 指数和总体自我评估健康)进行测量。6 个月的随访数据包括 QoL、住院和死亡率。使用配对 t 检验评估 QoL 的变化。使用 Cox 回归评估 MCM 和透析患者的生存情况。
该队列包括 192 名透析患者和 89 名 MCM 患者。MCM 患者年龄较大(平均年龄 82±6 岁 vs. 75±7 岁,p<0.01),平均肾功能较好(eGFR 11.5±4.0 毫升/分钟/1.73 米 vs. 8.0±2.9 毫升/分钟/1.73 米,p<0.01)。两组之间的基线 QoL 没有显著差异。六个月后,透析组的 EQ-5D 指数没有显著改善,平均±标准误差(SE)为 0.026±0.014(p=0.10;无临床意义),但保守组有较小但有临床意义的下降:0.047±0.022(p<0.01;组间差异 p<0.01)。50%的透析患者发生住院治疗,而 24%的保守患者发生住院治疗(p<0.01)。在 80 岁以上的患者中,开始透析的透析患者与 MCM 患者相比,没有生存获益。
保守治疗患者的 QoL 略有下降,而透析患者的 QoL 没有变化。然而,透析患者的住院率较高。在 80 岁以上的患者中,没有发现生存获益。