Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Republic of Korea; Department of Obstetrics and Gynecology, Seoul National University Bundang Hospital, Seongnam-si, Republic of Korea.
Perinatology Research Branch, NICHD/NIH/DHHS, Bethesda, MD, and Detroit, MI; Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI; Department of Epidemiology and Biostatistics, Michigan State University, East Lansing, MI; Center for Molecular Medicine and Genetics, Wayne State University, Detroit, MI.
Am J Obstet Gynecol. 2019 Aug;221(2):140.e1-140.e18. doi: 10.1016/j.ajog.2019.03.017. Epub 2019 Mar 28.
Cervical insufficiency is a risk factor for spontaneous midtrimester abortion or early preterm birth. Intra-amniotic infection has been reported in 8-52% of such patients and intra-amniotic inflammation in 81%. Some professional organizations have recommended perioperative antibiotic treatment when emergency cervical cerclage is performed. The use of prophylactic antibiotics is predicated largely on the basis that they reduce the rate of complications during the course of vaginal surgery. However, it is possible that antibiotic administration can also eradicate intra-amniotic infection/inflammation and improve pregnancy outcome.
To describe the outcome of antibiotic treatment in patients with cervical insufficiency and intra-amniotic infection/inflammation.
The study population consisted of 22 women who met the following criteria: (1) singleton pregnancy; (2) painless cervical dilatation of >1 cm between 16.0 and 27.9 weeks of gestation; (3) intact membranes and absence of uterine contractions; (4) transabdominal amniocentesis performed for the evaluation of the microbiologic and inflammatory status of the amniotic cavity; (5) presence of intra-amniotic infection/inflammation; and (6) antibiotic treatment (regimen consisted of ceftriaxone, clarithromycin, and metronidazole). Amniotic fluid was cultured for aerobic and anaerobic bacteria and genital mycoplasmas, and polymerase chain reaction for Ureaplasma spp. was performed. Intra-amniotic infection was defined as a positive amniotic fluid culture for microorganisms or a positive polymerase chain reaction for Ureaplasma spp., and intra-amniotic inflammation was suspected when there was an elevated amniotic fluid white blood cell count (≥19 cells/mm) or a positive rapid test for metalloproteinase-8 (sensitivity 10 ng/mL). For the purpose of this study, the "gold standard" for diagnosis of intra-amniotic inflammation was an elevated interleukin-6 concentration (>2.6 ng/mL) using an enzyme-linked immunosorbent assay. The results of amniotic fluid interleukin-6 were not available to managing clinicians. Follow-up amniocentesis was routinely offered to monitor the microbiologic and inflammatory status of the amniotic cavity and fetal lung maturity. Treatment success was defined as resolution of intra-amniotic infection/inflammation or delivery ≥34 weeks of gestation.
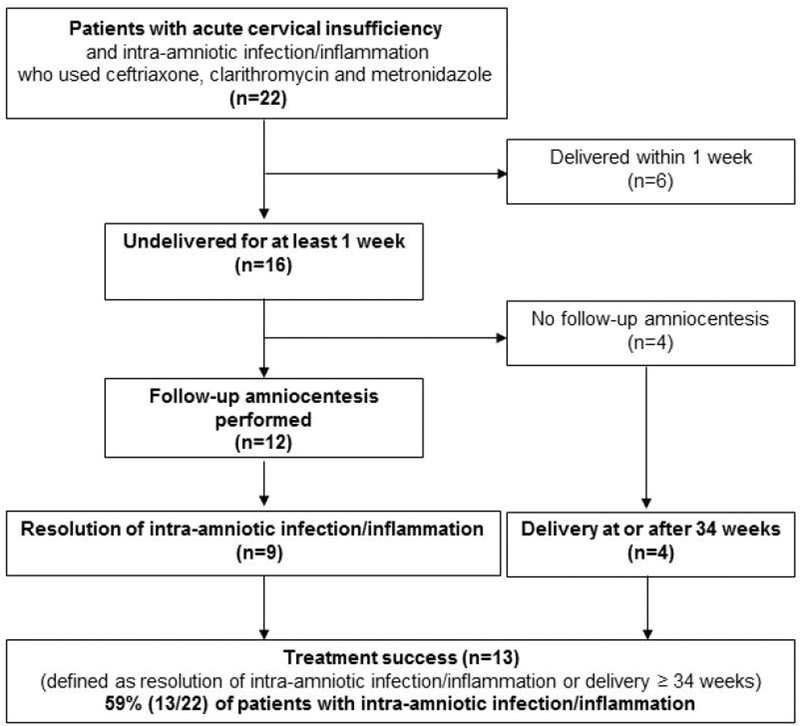
Of 22 patients with cervical insufficiency and intra-amniotic infection/inflammation, 3 (14%) had microorganisms in the amniotic fluid. Of the 22 patients, 6 (27%) delivered within 1 week of amniocentesis and the remaining 16 (73%) delivered more than 1 week after the diagnostic procedure. Among these, 12 had a repeat amniocentesis to assess the microbial and inflammatory status of the amniotic cavity; in 75% (9/12), there was objective evidence of resolution of intra-amniotic inflammation or intra-amniotic infection demonstrated by analysis of amniotic fluid at the time of the repeat amniocentesis. Of the 4 patients who did not have a follow-up amniocentesis, all delivered ≥34 weeks, 2 of them at term; thus, treatment success occurred in 59% (13/22) of cases.
In patients with cervical insufficiency and intra-amniotic infection/inflammation, administration of antibiotics (ceftriaxone, clarithromycin, and metronidazole) was followed by resolution of the intra-amniotic inflammatory process or intra-amniotic infection in 75% of patients and was associated with treatment success in about 60% of cases.
宫颈机能不全是自发性中期流产或早产的危险因素。据报道,此类患者中有 8-52%存在羊膜内感染,81%存在羊膜内炎症。一些专业组织建议在紧急宫颈环扎术时进行围手术期抗生素治疗。预防性使用抗生素主要基于它们可以降低阴道手术过程中并发症的发生率。然而,抗生素的使用也有可能消除羊膜内感染/炎症,改善妊娠结局。
描述宫颈机能不全伴羊膜内感染/炎症患者的抗生素治疗结果。
研究人群包括 22 名符合以下标准的女性:(1)单胎妊娠;(2)16.0 至 27.9 孕周无痛性宫颈扩张>1 厘米;(3)胎膜完整,无子宫收缩;(4)进行经腹羊膜穿刺术评估羊膜腔的微生物和炎症状态;(5)存在羊膜内感染/炎症;(6)抗生素治疗(方案包括头孢曲松、克拉霉素和甲硝唑)。对羊水进行需氧和厌氧菌以及生殖支原体培养,并进行解脲脲原体聚合酶链反应。羊膜内感染定义为微生物羊水培养阳性或解脲脲原体聚合酶链反应阳性,当羊水白细胞计数升高(≥19 个/毫米)或快速检测金属蛋白酶-8 阳性(灵敏度 10 纳克/毫升)时,怀疑存在羊膜内炎症。为了本研究的目的,羊膜内炎症的“金标准”诊断是使用酶联免疫吸附试验检测白细胞介素-6 浓度升高(>2.6 纳克/毫升)。管理临床医生无法获得羊水白细胞介素-6 的结果。常规进行随访羊膜穿刺术以监测羊膜腔的微生物和炎症状态以及胎儿肺成熟度。治疗成功定义为羊膜内感染/炎症的解决或≥34 孕周分娩。
在 22 例宫颈机能不全伴羊膜内感染/炎症的患者中,有 3 例(14%)羊水中有微生物。22 例患者中,6 例(27%)在羊膜穿刺术后 1 周内分娩,其余 16 例(73%)在诊断后 1 周以上分娩。其中 12 例患者进行了重复羊膜穿刺术以评估羊膜腔的微生物和炎症状态;在 12 例患者中,有 75%(9/12)通过重复羊膜穿刺术时的羊水分析显示羊膜内炎症或羊膜内感染有客观证据得到解决。在未进行随访羊膜穿刺术的 4 例患者中,均在≥34 孕周分娩,其中 2 例在足月分娩;因此,治疗成功率为 59%(13/22)。
在宫颈机能不全伴羊膜内感染/炎症的患者中,使用抗生素(头孢曲松、克拉霉素和甲硝唑)后,75%的患者羊膜内炎症过程或羊膜内感染得到解决,约 60%的患者治疗成功。