European Foundation for the Study of Chronic Liver Failure, Barcelona, Spain.
Department of Internal Medicine I, University of Bonn, Bonn, Germany.
Front Immunol. 2019 Mar 19;10:476. doi: 10.3389/fimmu.2019.00476. eCollection 2019.
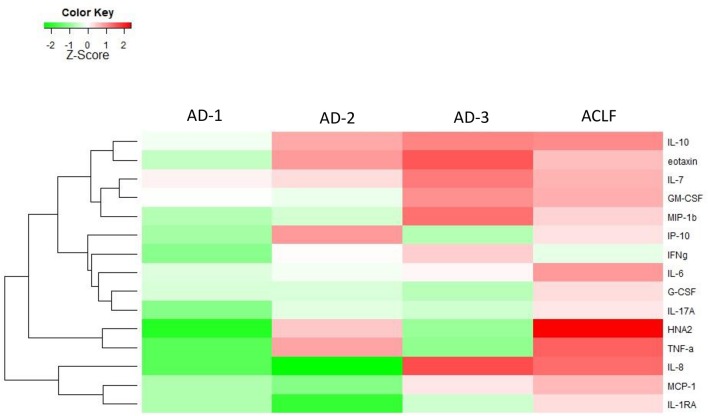
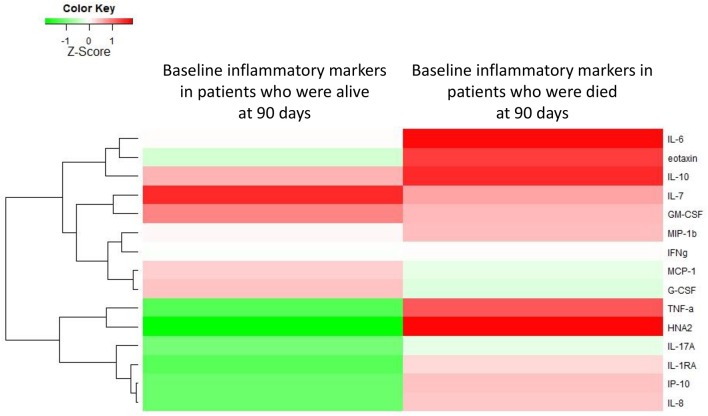
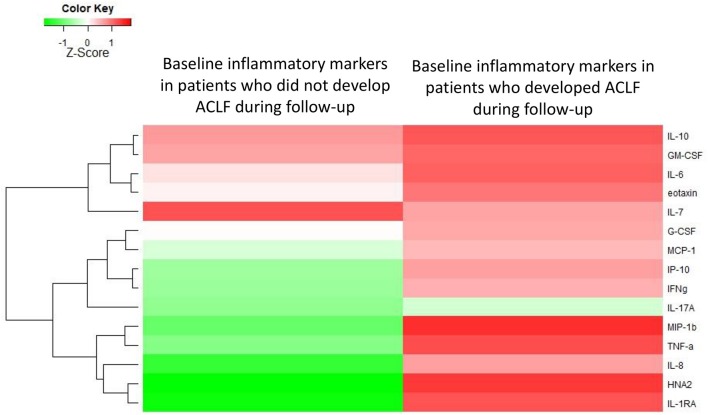
Patients with acutely decompensated cirrhosis (AD) may or may not develop acute-on-chronic liver failure (ACLF). ACLF is characterized by high-grade systemic inflammation, organ failures (OF) and high short-term mortality. Although patients with AD cirrhosis exhibit distinct clinical phenotypes at baseline, they have low short-term mortality, unless ACLF develops during follow-up. Because little is known about the association of profile of systemic inflammation with clinical phenotypes of patients with AD cirrhosis, we aimed to investigate a battery of markers of systemic inflammation in these patients. Upon hospital admission baseline plasma levels of 15 markers (cytokines, chemokines, and oxidized albumin) were measured in 40 healthy controls, 39 compensated cirrhosis, 342 AD cirrhosis, and 161 ACLF. According to EASL-CLIF criteria, AD cirrhosis was divided into three distinct clinical phenotypes (AD-1: Creatinine<1.5, no HE, no OF; AD-2: creatinine 1.5-2, and or HE grade I/II, no OF; AD-3: Creatinine<1.5, no HE, non-renal OF). Most markers were slightly abnormal in compensated cirrhosis, but markedly increased in AD. Patients with ACLF exhibited the largest number of abnormal markers, indicating "full-blown" systemic inflammation (all markers). AD-patients exhibited distinct systemic inflammation profiles across three different clinical phenotypes. In each phenotype, activation of systemic inflammation was only partial (30% of the markers). Mortality related to each clinical AD-phenotype was significantly lower than mortality associated with ACLF ( < 0.0001 by gray test). Among AD-patients baseline systemic inflammation (especially IL-8, IL-6, IL-1ra, HNA2 independently associated) was more intense in those who had poor 28-day outcomes (ACLF, death) than those who did not experience these outcomes. Although AD-patients exhibit distinct profiles of systemic inflammation depending on their clinical phenotypes, all these patients have only partial activation of systemic inflammation. However, those with the most extended baseline systemic inflammation had the highest the risk of ACLF development and death.
急性失代偿性肝硬化(AD)患者可能会也可能不会发展为慢加急性肝衰竭(ACLF)。ACLF 的特征是高级别的全身炎症、器官衰竭(OF)和高短期死亡率。尽管 AD 肝硬化患者在基线时表现出明显不同的临床表型,但除非在随访过程中发生 ACLF,否则他们的短期死亡率较低。由于人们对 AD 肝硬化患者全身炎症表型与临床表型的相关性知之甚少,我们旨在研究这些患者一系列全身炎症标志物。
在入院时,在 40 名健康对照者、39 名代偿性肝硬化患者、342 名 AD 肝硬化患者和 161 名 ACLF 患者中测量了基线血浆中 15 种标志物(细胞因子、趋化因子和氧化白蛋白)的水平。根据 EASL-CLIF 标准,AD 肝硬化分为三种不同的临床表型(AD-1:肌酐<1.5,无 HE,无 OF;AD-2:肌酐 1.5-2,且或 HE 分级 I/II,无 OF;AD-3:肌酐<1.5,无 HE,非肾 OF)。
大多数标志物在代偿性肝硬化中略有异常,但在 AD 中明显增加。ACLF 患者表现出最多数量的异常标志物,表明存在“全面”全身炎症(所有标志物)。AD 患者在三种不同的临床表型中表现出不同的全身炎症谱。在每种表型中,全身炎症的激活都是部分的(30%的标志物)。与每个临床 AD 表型相关的死亡率明显低于与 ACLF 相关的死亡率(灰色检验<0.0001)。在 AD 患者中,基线全身炎症(尤其是与 IL-8、IL-6、IL-1ra、HNA2 独立相关)在那些 28 天预后不良(ACLF、死亡)的患者中比那些没有经历这些结局的患者更强。
尽管 AD 患者根据其临床表型表现出不同的全身炎症谱,但所有这些患者的全身炎症仅部分激活。然而,那些基线全身炎症最严重的患者发生 ACLF 发展和死亡的风险最高。