Department of Orthopaedic Surgery, Osaka University, Graduate School of Medicine, Osaka, Japan.
Department of Advanced Medicine for Rheumatic Diseases, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Arthritis Res Ther. 2019 Apr 11;21(1):91. doi: 10.1186/s13075-019-1880-4.
The aim of this study is to evaluate the retention rates and reasons for discontinuation for seven biological disease-modifying antirheumatic drugs (bDMARDs) in a real-world setting of patients with rheumatoid arthritis (RA).
This multi-center, retrospective study assessed 4466 treatment courses of 2494 patients with bDMARDs from 2009 to 2017 (females, 82.4%; baseline age, 57.4 years; disease duration 8.5 years; rheumatoid factor positivity 78.6%; Disease Activity Score in 28 joints using erythrocyte sedimentation rate, 4.3; concomitant prednisolone (PSL) 2.7 mg/day (43.1%) and methotrexate (MTX) 5.0 mg/week (61.8%); and 63.6% patients were bio-naïve). Treatment courses included tocilizumab (TCZ; n = 895), etanercept (ETN; n = 891), infliximab (IFX; n = 748), abatacept (ABT; n = 681), adalimumab (ADA; n = 558), golimumab (GLM; n = 464), and certolizumab pegol (CZP; n = 229). Drug retention rates and discontinuation reasons were estimated at 36 months using the Kaplan-Meier method and adjusted for potential confounders (age, sex, disease duration, concomitant PSL and MTX, and switched number of bDMARDs) using Cox proportional hazards modeling.
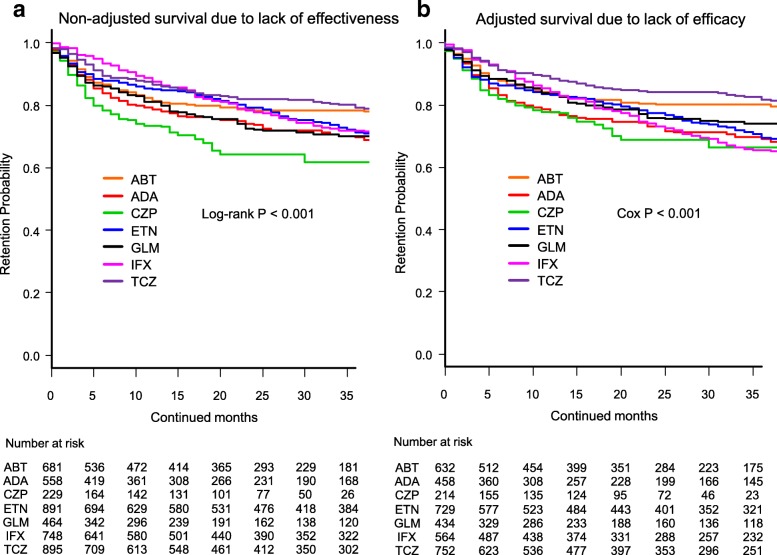
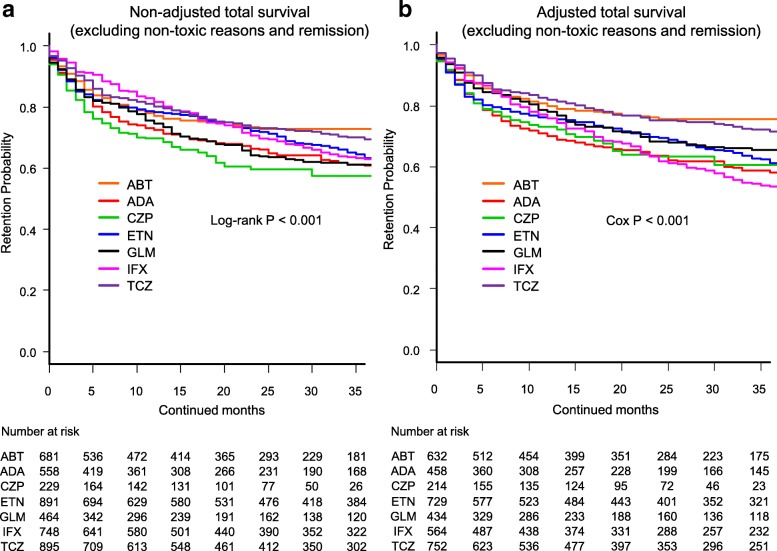
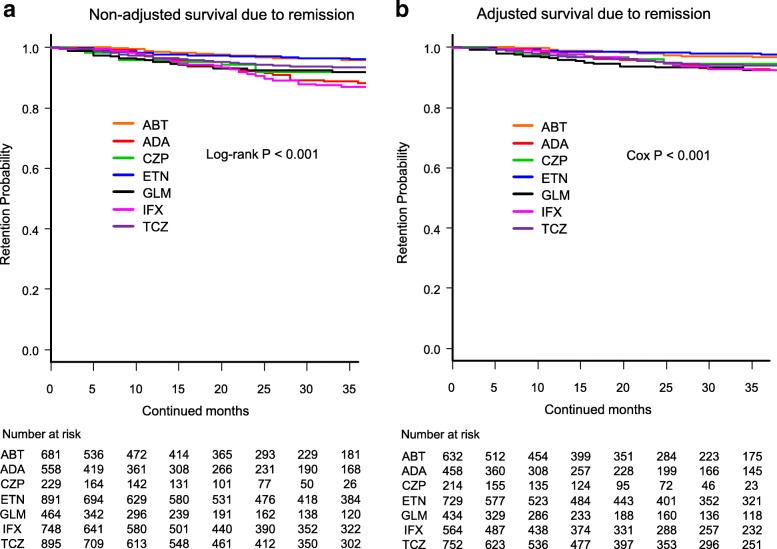
A total of 56.9% of treatment courses were stopped, with 25.8% stopping due to lack of effectiveness, 12.7% due to non-toxic reasons, 11.9% due to toxic adverse events, and 6.4% due to disease remission. Drug retention rates for each discontinuation reason were as follows: lack of effectiveness [from 65.5% (IFX) to 81.7% (TCZ); with significant differences between groups (Cox P < 0.001)], toxic adverse events [from 81.8% (IFX) to 94.0% (ABT), Cox P < 0.001], and remission [from 92.4% (ADA and IFX) to 97.7% (ETN), Cox P < 0.001]. Finally, overall retention rates excluding non-toxic reasons and remission for discontinuation ranged from 53.4% (IFX) to 75.5% (ABT) (Cox P < 0.001).
TCZ showed the lowest discontinuation rate by lack of effectiveness, ABT showed the lowest discontinuation rate by toxic adverse events, ADA and IFX showed the highest discontinuation rate by remission, and ABT showed the highest overall retention rates (excluding non-toxic reasons and remission) among seven bDMARDs in the adjusted model.
本研究旨在评估七种生物改善病情抗风湿药物(bDMARDs)在类风湿关节炎(RA)真实世界环境中的患者保留率和停药原因。
这项多中心、回顾性研究评估了 2009 年至 2017 年期间 2494 名患者的 4466 例 bDMARD 治疗疗程(女性占 82.4%;基线年龄为 57.4 岁;疾病病程为 8.5 年;类风湿因子阳性率为 78.6%;红细胞沉降率 28 关节疾病活动度评分 4.3;同时使用泼尼松龙(PSL)2.7mg/天(43.1%)和甲氨蝶呤(MTX)5.0mg/周(61.8%);63.6%的患者为生物初治)。治疗疗程包括托珠单抗(TCZ;n=895)、依那西普(ETN;n=891)、英夫利昔单抗(IFX;n=748)、阿巴西普(ABT;n=681)、阿达木单抗(ADA;n=558)、戈利木单抗(GLM;n=464)和培塞利珠单抗(CZP;n=229)。采用 Kaplan-Meier 法在 36 个月时估计药物保留率和停药原因,并使用 Cox 比例风险模型对潜在混杂因素(年龄、性别、疾病病程、同时使用 PSL 和 MTX 以及 bDMARDs 的转换数量)进行调整。
共有 56.9%的治疗疗程停止,其中 25.8%因缺乏疗效而停药,12.7%因非毒性原因停药,11.9%因毒性不良反应停药,6.4%因疾病缓解而停药。每个停药原因的药物保留率如下:缺乏疗效[IFX 为 65.5%(IFX)至 81.7%(TCZ);组间差异有统计学意义(Cox P<0.001)]、毒性不良反应[IFX 为 81.8%(IFX)至 94.0%(ABT),Cox P<0.001]和缓解[ADA 和 IFX 为 92.4%(ADA 和 IFX)至 97.7%(ETN),Cox P<0.001]。最后,排除非毒性原因和缓解的总体保留率范围为 IFX 为 53.4%(IFX)至 ABT 为 75.5%(ABT)(Cox P<0.001)。
TCZ 因缺乏疗效导致停药率最低,ABT 因毒性不良反应导致停药率最低,ADA 和 IFX 因缓解导致停药率最高,ABT 因排除非毒性原因和缓解的总体保留率最高(调整模型)。