Mechie Nicolae-Catalin, Mavropoulou Eirini, Ellenrieder Volker, Petzold Golo, Kunsch Steffen, Neesse Albrecht, Amanzada Ahmad
University Medical Center Göttingen, Department of Gastroenterology and Gastrointestinal Oncology, Robert- Koch-Str., Göttingen, Germany.
Medicine (Baltimore). 2019 Apr;98(15):e15172. doi: 10.1097/MD.0000000000015172.
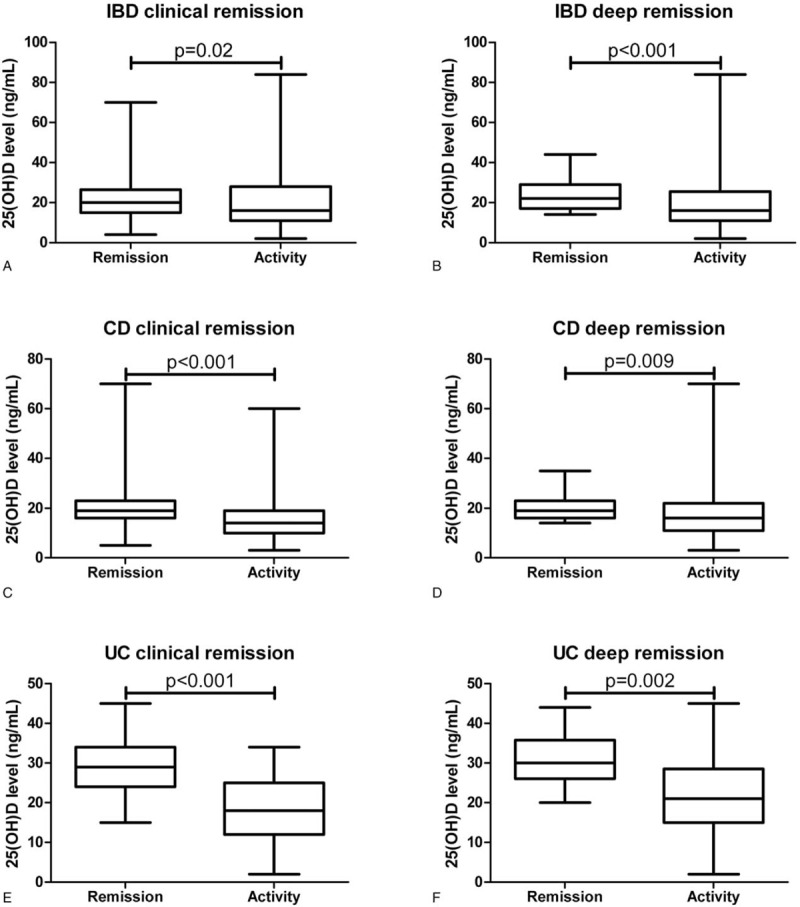
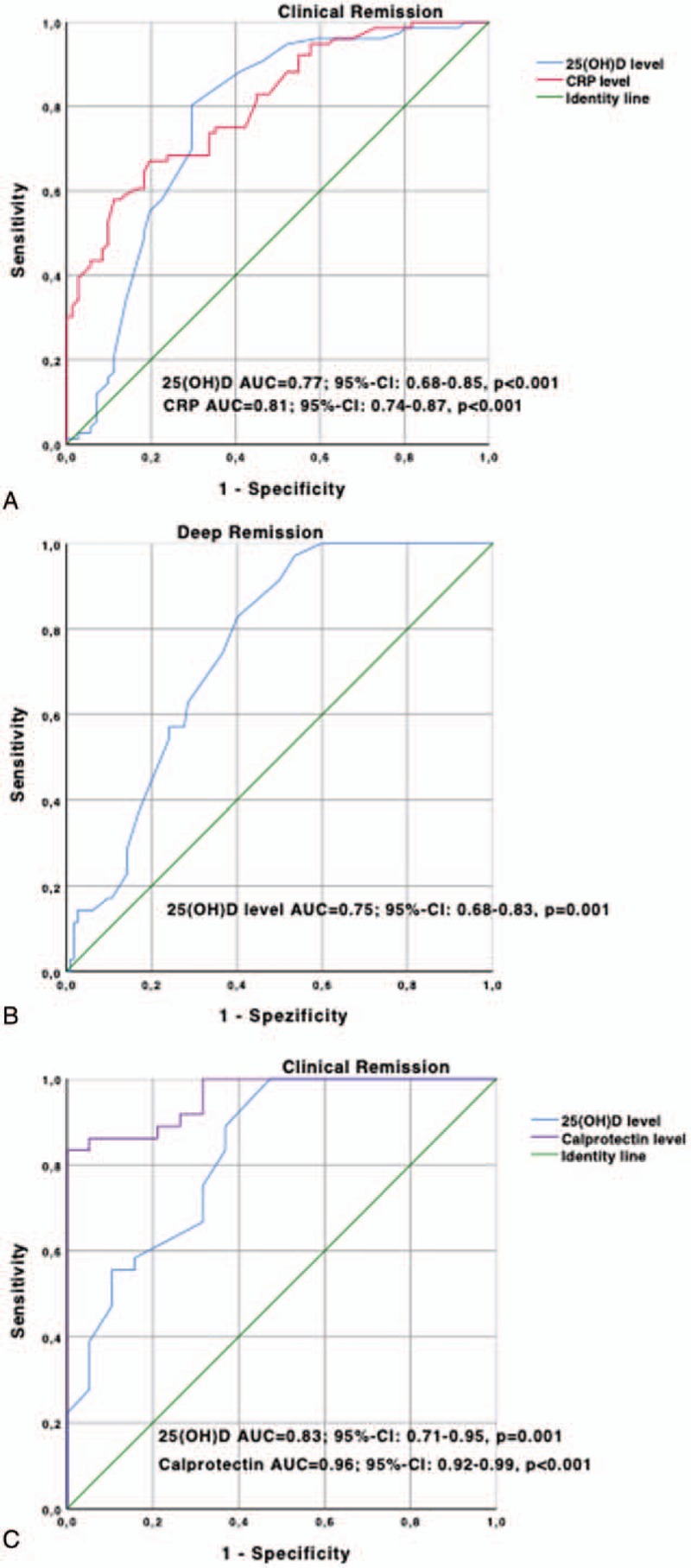
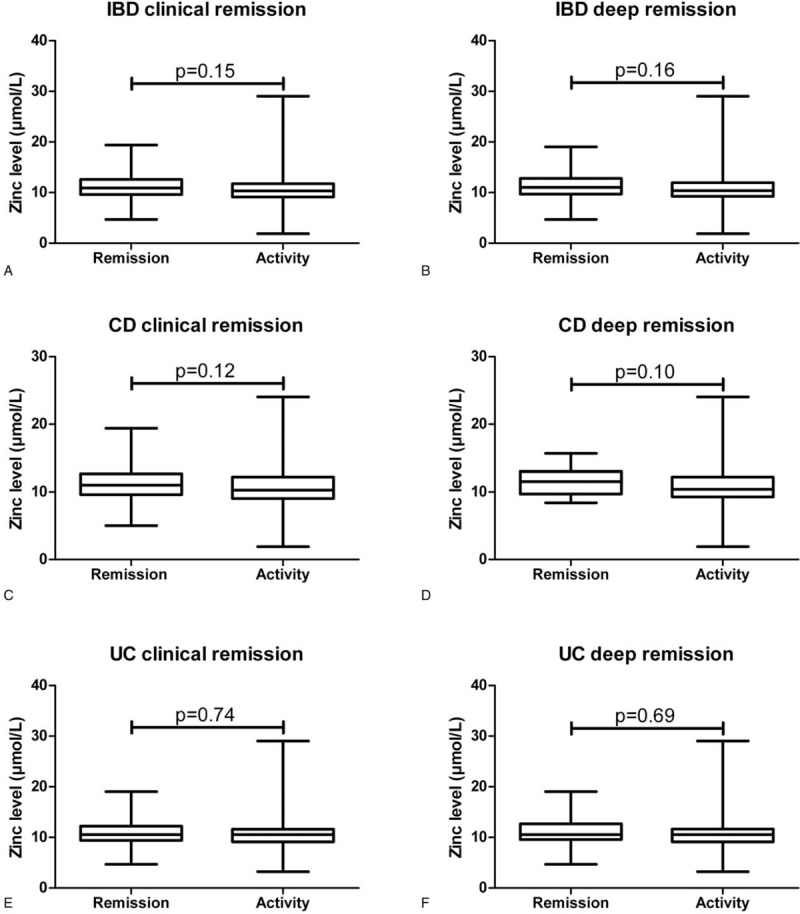
The incidence of inflammatory bowel disease (IBD) is increasing and the pathogenesis is still not completely understood. Micronutrients like vitamin D [25 (OH)D] and zinc play an important role in enzyme activities and the immune system. As the 25 (OH)D-receptor has been shown to be downregulated in patients with IBD, 25 (OH)D may emerge as a predictive marker for disease improvement. Studies on relationship of both micronutrients in IBD patients are lacking.We retrospectively evaluated serum levels of 25(OH)D and zinc together with baseline characteristics of 232 IBD patients. Uni- and multivariate analyses were performed for association between serum levels of 25(OH)D and zinc with clinical and deep remission (CR and DR).155 Crohn's disease (CD) and 77 ulcerative colitis (UC) patients were included. 54% (n = 125) and 6% (n = 14) of IBD patients showed deficient serum 25(OH)D levels below 20 ng/mL and zinc levels below 7 μmol/L. Serum 25(OH)D levels were significantly higher in IBD patients with CR (P = .02) and DR (P < .001) but not serum zinc levels, respectively. Serum 25(OH)D levels (P = .008), anti-tumor-necrosis-factor-α-trough-concentration (anti-TNF-α-TC) (P = .02) and CRP level (P = .02) were independently associated with CR in CD patients. Serum 25(OH)D threshold of 19 ng/mL discriminated CD patients with or without CR, having an area under the receiver operating curve analysis (AUROC) of 0.77 [95%-confidence interval (CI): 0.68-0.85]. In multivariate analysis serum 25(OH)D levels (P = .04) and anti-TNF-α-TC (P = .04) were associated with DR in CD patients. Serum 25(OH)D threshold of 26 ng/mL discriminated CD patients with or without DR, having an AUROC of 0.75 (95%-CI: 0.68-0.83).Serum 25(OH)D (P = .04) and fecal calprotectin levels (P = .04) were independently correlated with CR in UC patients. Serum 25(OH)D threshold of 32 ng/mL discriminated UC patients in CR with an AUROC of 0.83 (95%-CI: 0.71-0.95). Zinc levels did not correlate with disease activity status in CD or UC patients either.In conclusion, beside CRP and fecal calprotectin, serum 25(OH)D levels, but not serum zinc levels, may be an additional useful and noninvasive marker for characterizing different disease activity status of IBD patients. Measurement of serum 25(OH)D in IBD patients may be warranted. 25(OH)D supplementation in deficient IBD patients is recommended.
炎症性肠病(IBD)的发病率正在上升,但其发病机制仍未完全明确。维生素D[25(OH)D]和锌等微量营养素在酶活性和免疫系统中发挥着重要作用。由于IBD患者的25(OH)D受体已被证明下调,25(OH)D可能成为疾病改善的预测标志物。目前缺乏关于IBD患者中这两种微量营养素关系的研究。我们回顾性评估了232例IBD患者的血清25(OH)D和锌水平以及基线特征。对25(OH)D和锌的血清水平与临床和深度缓解(CR和DR)之间的关联进行了单因素和多因素分析。纳入了155例克罗恩病(CD)患者和77例溃疡性结肠炎(UC)患者。54%(n = 125)的IBD患者血清25(OH)D水平低于20 ng/mL,6%(n = 14)的患者血清锌水平低于7 μmol/L,呈现缺乏状态。IBD患者中达到CR(P = 0.02)和DR(P < 0.001)的患者血清25(OH)D水平显著更高,但血清锌水平并非如此。血清25(OH)D水平(P = 0.008)、抗肿瘤坏死因子-α谷浓度(抗TNF-α-TC)(P = 0.02)和CRP水平(P = 0.02)与CD患者的CR独立相关。19 ng/mL的血清25(OH)D阈值可区分有或无CR的CD患者,在受试者工作特征曲线分析(AUROC)中的曲线下面积为0.77[95%置信区间(CI):0.68 - 0.85]。在多因素分析中,血清25(OH)D水平(P = 0.04)和抗TNF-α-TC(P = 0.04)与CD患者的DR相关。26 ng/mL的血清25(OH)D阈值可区分有或无DR的CD患者,AUROC为0.75(95%CI:0.68 - 0.83)。血清25(OH)D(P = 0.04)和粪便钙卫蛋白水平(P = 0.04)与UC患者的CR独立相关。32 ng/mL的血清25(OH)D阈值可区分处于CR的UC患者,AUROC为0.83(95%CI:0.71 - 0.95)。锌水平与CD或UC患者的疾病活动状态均无相关性。总之,除了CRP和粪便钙卫蛋白外,血清25(OH)D水平而非血清锌水平,可能是用于表征IBD患者不同疾病活动状态额外有用且无创的标志物。对IBD患者进行血清25(OH)D检测可能是必要的。建议对缺乏25(OH)D的IBD患者进行补充。