Fergusson Nicholas A, Ramsay Tim, Chassé Michaël, English Shane W, Knoll Greg A
School of Epidemiology and Public Health, University of Ottawa, Ottawa, Canada.
Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, Canada.
Transplant Direct. 2019 Mar 19;5(4):e439. doi: 10.1097/TXD.0000000000000880. eCollection 2019 Apr.
Nephrology trials assessing the impact of interventions on "standard" outcomes, such as doubling of creatinine, end-stage renal disease (ESRD), and/or death, are difficult to conduct given the time required for endpoints to accrue. The objective of this study was to determine if using lesser declines in kidney function would alter the interpretation of a previous randomized controlled trial.
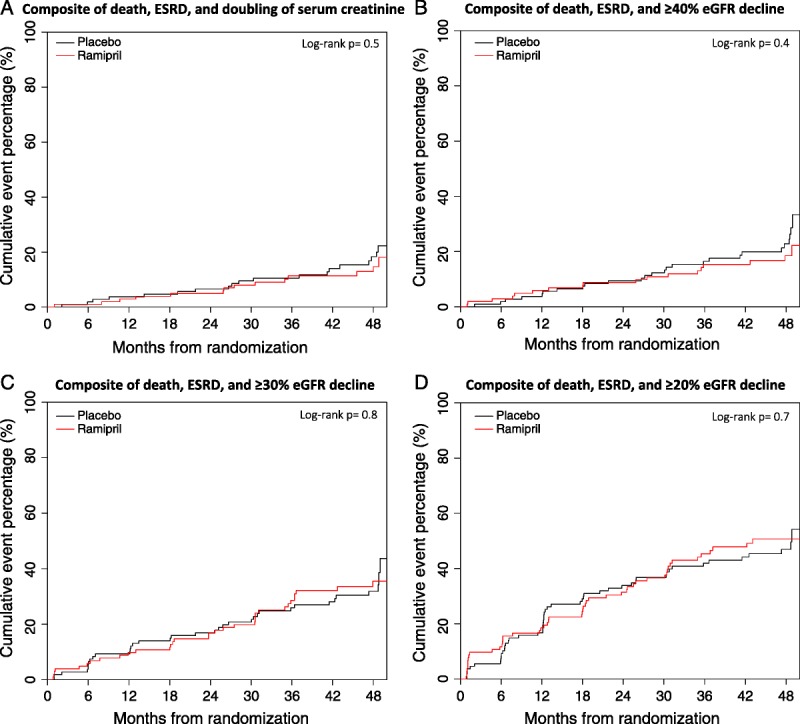
This study was a secondary analysis of a kidney transplant trial comparing the use of a 40% or greater, 30% or greater, or 20% or greater decline in estimated glomerular filtration rate (eGFR) as a substitute for doubling of serum creatinine. Declines in eGFR were determined relative to baseline. This trial enrolled 212 kidney transplant patients with proteinuria and assessed the clinical impact of ramipril versus placebo on a primary outcome of doubling of serum creatinine, ESRD, or death. In this analysis, the declines in eGFR replaced doubling of creatinine in the composite endpoint.
Mean trial follow-up was 41 months. A time-to-event composite of death, ESRD, or a 40% or greater, 30% or greater, or 20% or greater eGFR decline occurred in 45 (26 placebo vs 19 ramipril), 68 (35 vs 33), and 99 (50 vs 49) patients, respectively. Substituting these eGFR declines for doubling of serum creatinine resulted in an increase of 12, 35, and 66 endpoints compared with the original trial. In all 3 eGFR declines, ramipril treatment was not associated with any statistically significant differences despite the increase in events.
Substituting doubling of serum creatinine for lesser eGFR percentage decline thresholds did not alter trial interpretation but did increase the number of events.
鉴于终点事件的累积需要时间,评估干预措施对“标准”结局(如肌酐翻倍、终末期肾病(ESRD)和/或死亡)影响的肾脏病学试验很难开展。本研究的目的是确定使用较小的肾功能下降幅度是否会改变对先前一项随机对照试验的解读。
本研究是一项肾移植试验的二次分析,该试验比较了使用估计肾小球滤过率(eGFR)下降40%及以上、30%及以上或20%及以上作为血清肌酐翻倍的替代指标。eGFR下降是相对于基线确定的。该试验纳入了212例有蛋白尿的肾移植患者,并评估了雷米普利与安慰剂对血清肌酐翻倍、ESRD或死亡这一主要结局的临床影响。在本次分析中,eGFR下降替代了复合终点中的肌酐翻倍。
试验平均随访时间为41个月。分别有45例(26例使用安慰剂,19例使用雷米普利)、68例(35例使用安慰剂,33例使用雷米普利)和99例(50例使用安慰剂,49例使用雷米普利)患者发生了死亡、ESRD或eGFR下降40%及以上、30%及以上或20%及以上的事件复合终点。用这些eGFR下降替代血清肌酐翻倍,与原试验相比,终点事件分别增加了12例、35例和66例。在所有3种eGFR下降情况中,尽管事件增加,但雷米普利治疗与任何统计学上的显著差异均无关联。
用血清肌酐翻倍替代较小的eGFR下降百分比阈值并未改变试验解读,但确实增加了事件数量。