Renal Division, Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
Pathology Division, Department of Molecular and Cell Based Medicine, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
Kidney Int. 2022 Feb;101(2):288-298. doi: 10.1016/j.kint.2021.09.028. Epub 2021 Oct 30.
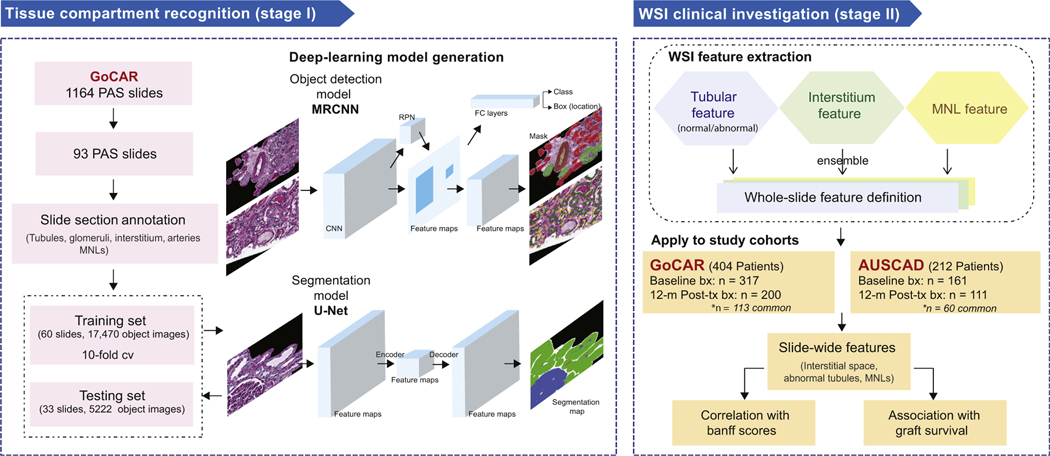
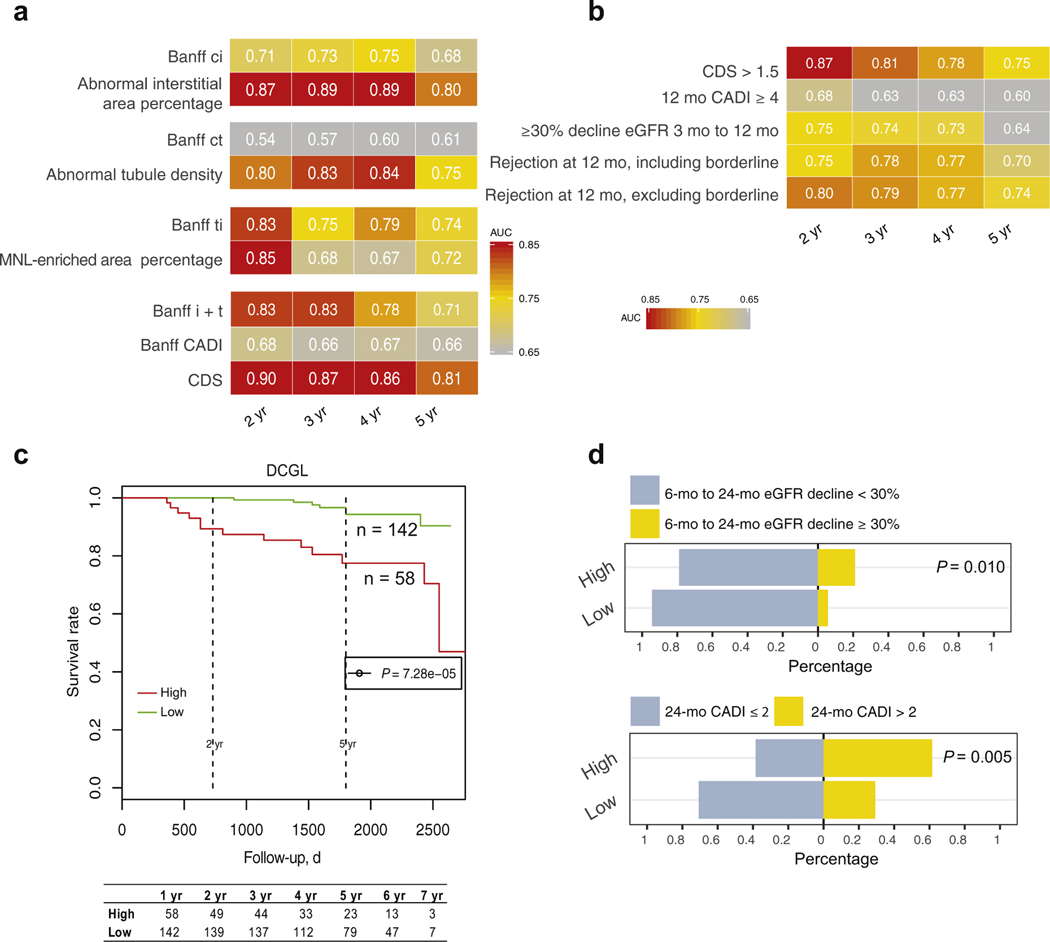
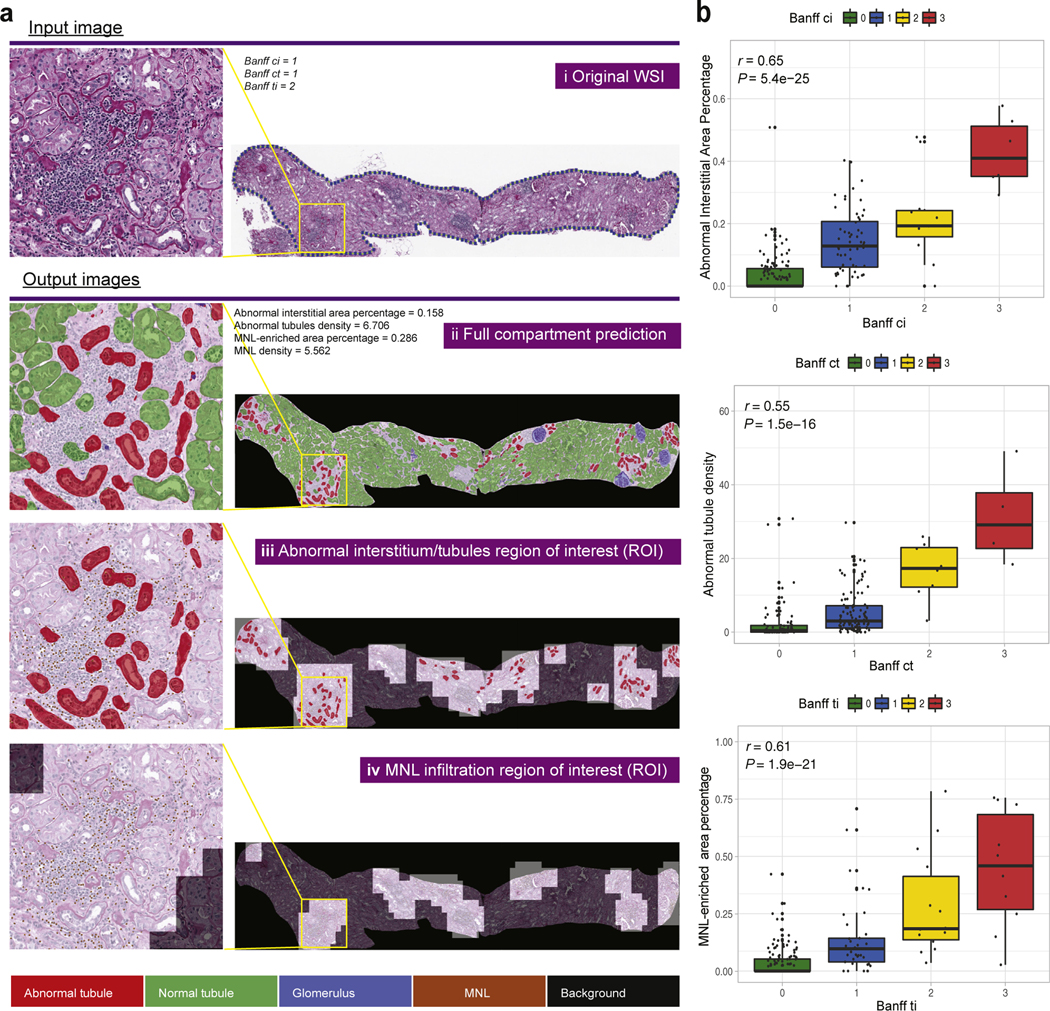
Interstitial fibrosis, tubular atrophy, and inflammation are major contributors to kidney allograft failure. Here we sought an objective, quantitative pathological assessment of these lesions to improve predictive utility and constructed a deep-learning-based pipeline recognizing normal vs. abnormal kidney tissue compartments and mononuclear leukocyte infiltrates. Periodic acid- Schiff stained slides of transplant biopsies (60 training and 33 testing) were used to quantify pathological lesions specific for interstitium, tubules and mononuclear leukocyte infiltration. The pipeline was applied to the whole slide images from 789 transplant biopsies (478 baseline [pre-implantation] and 311 post-transplant 12-month protocol biopsies) in two independent cohorts (GoCAR: 404 patients, AUSCAD: 212 patients) of transplant recipients to correlate composite lesion features with graft loss. Our model accurately recognized kidney tissue compartments and mononuclear leukocytes. The digital features significantly correlated with revised Banff 2007 scores but were more sensitive to subtle pathological changes below the thresholds in the Banff scores. The Interstitial and Tubular Abnormality Score (ITAS) in baseline samples was highly predictive of one-year graft loss, while a Composite Damage Score in 12-month post-transplant protocol biopsies predicted later graft loss. ITASs and Composite Damage Scores outperformed Banff scores or clinical predictors with superior graft loss prediction accuracy. High/intermediate risk groups stratified by ITASs or Composite Damage Scores also demonstrated significantly higher incidence of estimated glomerular filtration rate decline and subsequent graft damage. Thus, our deep-learning approach accurately detected and quantified pathological lesions from baseline or post-transplant biopsies and demonstrated superior ability for prediction of post-transplant graft loss with potential application as a prevention, risk stratification or monitoring tool.
间质纤维化、肾小管萎缩和炎症是导致肾移植失败的主要因素。在这里,我们寻求一种客观的、定量的病理评估方法来提高预测的准确性,并构建了一个基于深度学习的模型,用于识别正常和异常的肾组织腔室以及单核白细胞浸润。使用过碘酸-希夫染色的移植活检切片(60 个训练和 33 个测试)来定量分析间质、肾小管和单核白细胞浸润的特定病变。该模型应用于两个独立队列(GoCAR:404 例患者,AUSCAD:212 例患者)的 789 例移植活检的全切片图像(478 例基线[移植前]和 311 例移植后 12 个月方案活检)中,以将复合病变特征与移植物丢失相关联。我们的模型准确地识别了肾组织腔室和单核白细胞。数字特征与修订后的 Banff 2007 评分显著相关,但对 Banff 评分阈值以下的细微病理变化更敏感。基线样本中的间质和肾小管异常评分(ITAS)对一年移植物丢失具有高度预测性,而移植后 12 个月方案活检中的复合损伤评分则预测了后期移植物丢失。ITAS 和复合损伤评分优于 Banff 评分或临床预测因子,具有更高的移植物丢失预测准确性。通过 ITAS 或复合损伤评分分层的高/中风险组也显示出肾小球滤过率下降和随后移植物损伤的发生率显著升高。因此,我们的深度学习方法可以准确地从基线或移植后活检中检测和定量病理病变,并具有卓越的预测移植后移植物丢失的能力,具有作为预防、风险分层或监测工具的潜在应用价值。