Department of Radiology, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China.
Korean J Radiol. 2019 May;20(5):791-800. doi: 10.3348/kjr.2018.0474.
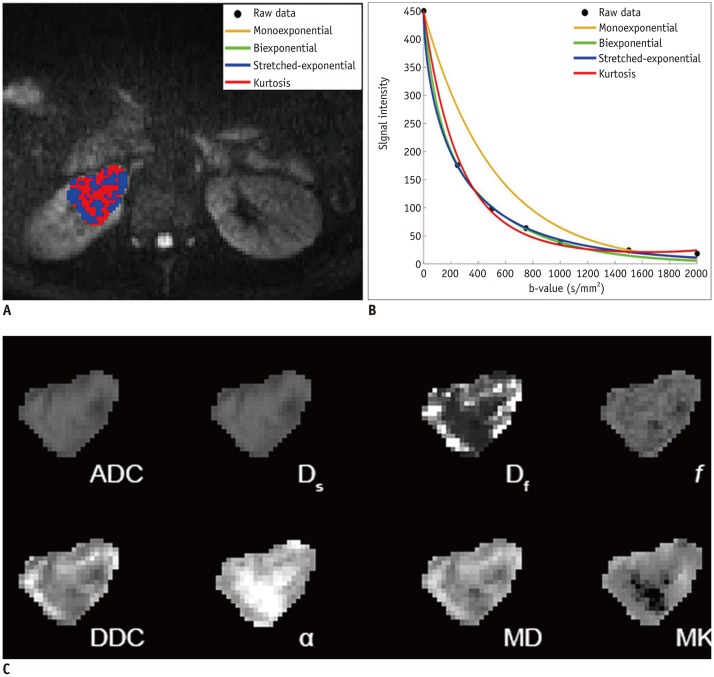
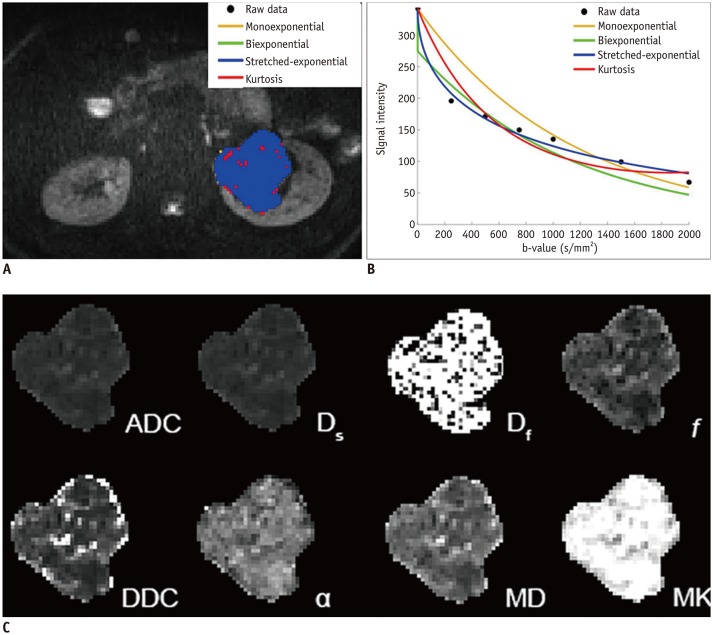
To compare various models of diffusion-weighted imaging including monoexponential apparent diffusion coefficient (ADC), biexponential (fast diffusion coefficient [D], slow diffusion coefficient [D], and fraction of fast diffusion), stretched-exponential (distributed diffusion coefficient and anomalous exponent term [α]), and kurtosis (mean diffusivity and mean kurtosis [MK]) models in the differentiation of renal solid masses.
A total of 81 patients (56 men and 25 women; mean age, 57 years; age range, 30-69 years) with 18 benign and 63 malignant lesions were imaged using 3T diffusion-weighted MRI. Diffusion model selection was investigated in each lesion using the Akaike information criteria. Mann-Whitney U test and receiver operating characteristic (ROC) analysis were used for statistical evaluations.
Goodness-of-fit analysis showed that the stretched-exponential model had the highest voxel percentages in benign and malignant lesions (90.7% and 51.4%, respectively). ADC, D, and MK showed significant differences between benign and malignant lesions ( < 0.05) and between low- and high-grade clear cell renal cell carcinoma (ccRCC) ( < 0.05). α was significantly lower in the benign group than in the malignant group ( < 0.05). All diffusion measures showed significant differences between ccRCC and non-ccRCC ( < 0.05) except D and α ( = 0.143 and 0.112, respectively). α showed the highest diagnostic accuracy in differentiating benign and malignant lesions with an area under the ROC curve of 0.923, but none of the parameters from these advanced models revealed significantly better performance over ADC in discriminating subtypes or grades of renal cell carcinoma (RCC) ( > 0.05).
Compared with conventional diffusion parameters, α may provide additional information for differentiating benign and malignant renal masses, while ADC remains the most valuable parameter for differentiation of RCC subtypes and for ccRCC grading.
比较各种扩散加权成像模型,包括单指数表观扩散系数(ADC)、双指数(快扩散系数[D]、慢扩散系数[D]和快扩散分数)、拉伸指数(分布扩散系数和异常指数项[α])和峰度(平均扩散系数和平均峰度[MK])模型,以区分肾脏实性肿块。
共对 81 例患者(男 56 例,女 25 例;平均年龄 57 岁;年龄范围 30-69 岁)的 18 个良性和 63 个恶性病变进行了 3T 扩散加权 MRI 成像。使用 Akaike 信息准则对每个病变的扩散模型选择进行了研究。采用 Mann-Whitney U 检验和受试者工作特征(ROC)分析进行统计学评估。
拟合优度分析显示,拉伸指数模型在良性和恶性病变中的体素百分比最高(分别为 90.7%和 51.4%)。ADC、D 和 MK 在良性和恶性病变之间(<0.05)以及低级别和高级别透明细胞肾细胞癌(ccRCC)之间(<0.05)有显著差异。α在良性组明显低于恶性组(<0.05)。除 D 和 α(分别为 0.143 和 0.112)外,所有扩散指标在 ccRCC 和非 ccRCC 之间均有显著差异(<0.05)。α在区分良恶性病变方面具有最高的诊断准确性,ROC 曲线下面积为 0.923,但这些高级模型的参数在区分肾细胞癌(RCC)亚型和分级方面均未显示出优于 ADC 的性能(>0.05)。
与常规扩散参数相比,α可能为区分良恶性肾肿块提供更多信息,而 ADC 仍然是区分 RCC 亚型和 ccRCC 分级的最有价值参数。