Kaiser Peter K, Kodjikian Laurent, Korobelnik Jean-Francois, Winkler Julia, Torri Albert, Zeitz Oliver, Vitti Robert, Ahlers Cristiane, Zimmermann Torsten, Dicioccio A Thomas, Höchel Joachim
Department of Ophthalmology, Cleveland Clinic Cole Eye Institute, Cleveland, Ohio, USA.
Department of Ophthalmology, Croix-Rousse Teaching Hospital, Hospices Civils de Lyon, UMR-CNRS 5510 Matéis, University of Medicine Lyon, Lyon, France.
BMJ Open Ophthalmol. 2019 Mar 20;4(1):e000185. doi: 10.1136/bmjophth-2018-000185. eCollection 2019.
Explore relationships between systemic exposure to intravitreal aflibercept injection (IAI) and systemic pharmacodynamic effects via post hoc analyses of clinical trials of IAI for neovascular age-related macular degeneration (nAMD) or diabetic macular oedema (DME).
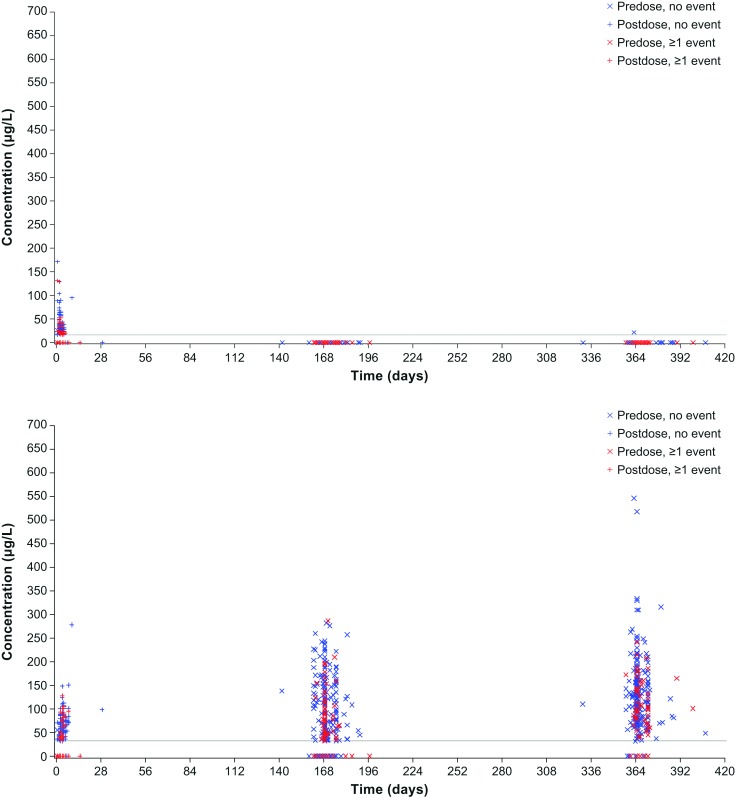
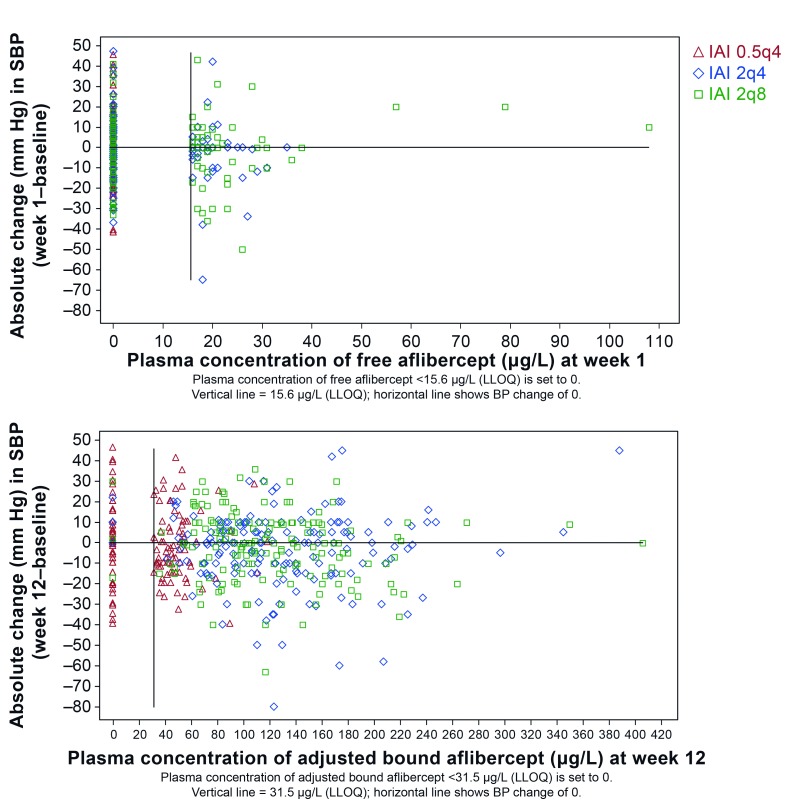
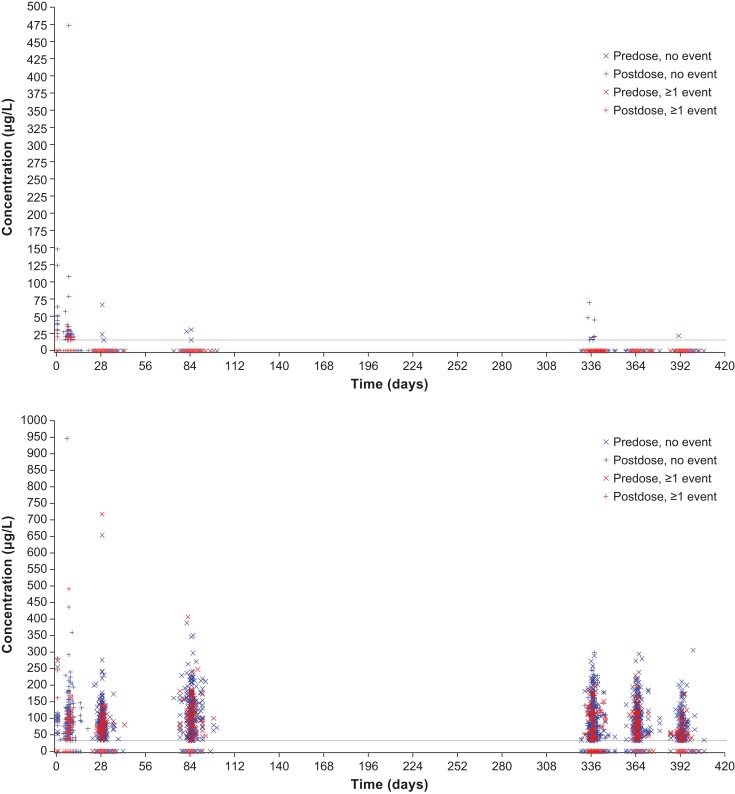
Adults from VGFT-OD-0702.PK (n=6), VGFT-OD-0512 (n= 5), VIEW 2 (n=1204) and VIVID-DME (n=404) studies were included. Validated ELISAs were used to measure concentrations of free and bound aflibercept (reported as adjusted bound) in plasma at predefined time points in each study. Non-compartmental analysis of concentration-time data was obtained with dense sampling in VGFT-OD-0702.PK and VGFT-OD-0512. Sparse sampling was used in VIEW 2 and VIVID-DME. Blood pressure or intrarenal function changes were also investigated.
Following intravitreal administration, free aflibercept plasma concentrations quickly decreased once maximum concentrations were achieved at 1-3 days postdose; pharmacologically inactive adjusted bound aflibercept concentrations increased over a longer period and reached plateau 7 days postdose. Ratios of free and adjusted bound aflibercept decreased over time. There were no meaningful changes in systolic/diastolic blood pressure over the duration of each study at all systemic aflibercept exposure levels. For all treatment arms in VIEW 2, there was no clinically relevant change in mean intrarenal function from baseline at week 52. Overall, incidence of systemic adverse events in VIEW 2 and VIVID-DME was low and consistent with the known safety profile of IAI.
IAI administration was not associated with systemic effects in patients with nAMD or DME as measured by blood pressure or intrarenal function, two known pharmacologically relevant effects of anti-vascular endothelial growth factor.
通过对玻璃体内注射阿柏西普(IAI)治疗新生血管性年龄相关性黄斑变性(nAMD)或糖尿病性黄斑水肿(DME)的临床试验进行事后分析,探讨全身暴露于IAI与全身药效学效应之间的关系。
纳入来自VGFT-OD-0702.PK(n = 6)、VGFT-OD-0512(n = 5)、VIEW 2(n = 1204)和VIVID-DME(n = 404)研究的成年人。在每项研究的预定时间点,使用经过验证的酶联免疫吸附测定法(ELISA)测量血浆中游离和结合型阿柏西普的浓度(报告为调整后的结合型)。在VGFT-OD-0702.PK和VGFT-OD-0512中采用密集采样对浓度-时间数据进行非房室分析。VIEW 2和VIVID-DME采用稀疏采样。还研究了血压或肾内功能变化。
玻璃体内给药后,游离阿柏西普血浆浓度在给药后1 - 3天达到最大浓度后迅速下降;药理活性不高的调整后结合型阿柏西普浓度在较长时间内升高,并在给药后7天达到平台期。游离型与调整后结合型阿柏西普的比例随时间下降。在所有全身阿柏西普暴露水平下,每项研究期间收缩压/舒张压均无有意义的变化。对于VIEW 2的所有治疗组,在第52周时平均肾内功能与基线相比无临床相关变化。总体而言,VIEW 2和VIVID-DME中全身不良事件的发生率较低,与IAI已知的安全性特征一致。
通过血压或肾内功能测量,IAI给药与nAMD或DME患者的全身效应无关,而血压和肾内功能是抗血管内皮生长因子两种已知的药理相关效应。