Musculoskeletal Research Unit, Translational Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK.
Musculoskeletal Research Unit, Translational Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK; National Institute for Health Research Bristol Biomedical Research Centre, University Hospitals Bristol NHS Foundation Trust and University of Bristol, Bristol, UK.
Lancet Infect Dis. 2019 Jun;19(6):589-600. doi: 10.1016/S1473-3099(18)30755-2. Epub 2019 Apr 17.
Prosthetic joint infection is a devastating complication of knee replacement. The risk of developing a prosthetic joint infection is affected by patient, surgical, and health-care system factors. Existing evidence is limited by heterogeneity in populations studied, short follow-up, inadequate power, and does not differentiate early prosthetic joint infection, most likely related to the intervention, from late infection, more likely to occur due to haematogenous bacterial spread. We aimed to assess the overall and time-specific associations of these factors with the risk of revision due to prosthetic joint infection following primary knee replacement.
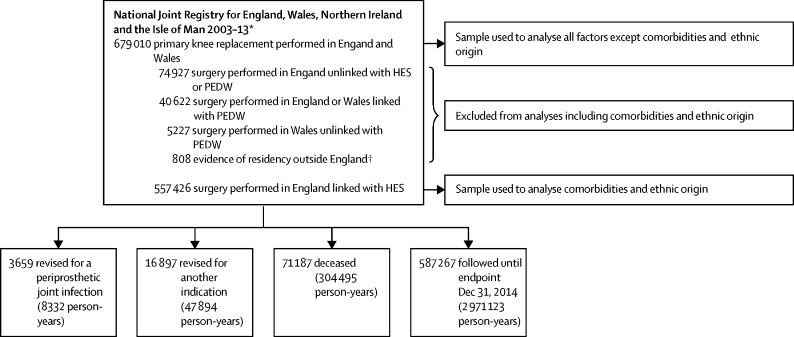
In this cohort study, we analysed primary knee replacements done between 2003 and 2013 in England and Wales and the procedures subsequently revised for prosthetic joint infection between 2003 and 2014. Data were obtained from the National Joint Registry linked to the Hospital Episode Statistics data in England and the Patient Episode Database for Wales. Each primary replacement was followed for a minimum of 12 months until the end of the observation period (Dec 31, 2014) or until the date of revision for prosthetic joint infection, revision for another indication, or death (whichever occurred first). We analysed the data using Poisson and piecewise exponential multilevel models to assess the associations between patient, surgical, and health-care system factors and risk of revision for prosthetic joint infection.
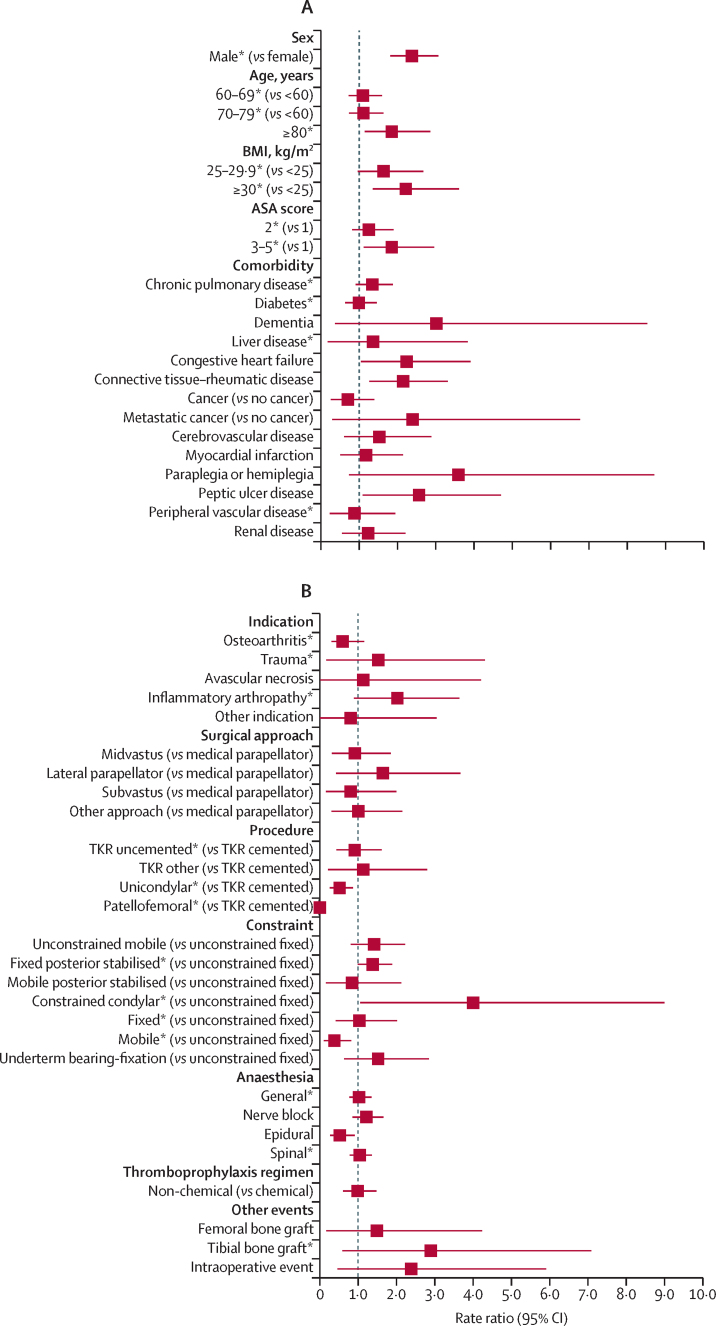
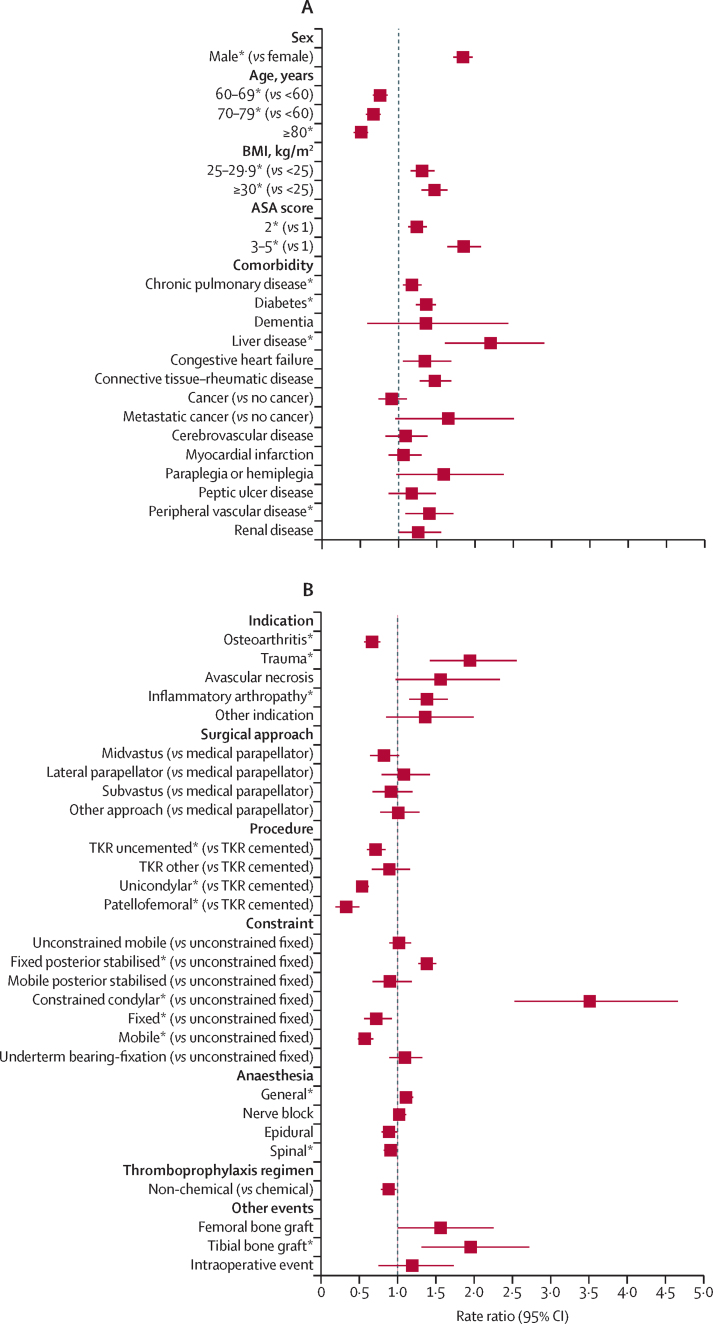
Of 679 010 primary knee replacements done between 2003 and 2013 in England and Wales, 3659 were subsequently revised for an indication of prosthetic joint infection between 2003 and 2014, after a median follow-up of 4·6 years (IQR 2·6-6·9). Male sex (rate ratio [RR] for male vs female patients 1·8 [95% CI 1·7-2·0]), younger age (RR for age ≥80 years vs <60 years 0·5 [0·4-0·6]), higher American Society of Anaesthesiologists [ASA] grade (RR for ASA grade 3-5 vs 1, 1·8 [1·6-2·1]), elevated body-mass index (BMI; RR for BMI ≥30 kg/mvs <25 kg/m 1·5 [1·3-1·6]), chronic pulmonary disease (RR 1·2 [1·1-1·3]), diabetes (RR 1·4 [1·2-1·5]), liver disease (RR 2·2 [1·6-2·9]), connective tissue and rheumatic diseases (RR 1·5 [1·3-1·7]), peripheral vascular disease (RR 1·4 [1·1-1·7]), surgery for trauma (RR 1·9 [1·4-2·6]), previous septic arthritis (RR 4·9 [2·7-7·6]) or inflammatory arthropathy (RR 1·4 [1·2-1·7]), operation under general anaesthesia (RR 1·1 [1·0-1·2]), requirement for tibial bone graft (RR 2·0 [1·3-2·7]), use of posterior stabilised fixed bearing prostheses (RR for posterior stabilised fixed bearing prostheses vs unconstrained fixed bearing prostheses 1·4 [1·3-1·5]) or constrained condylar prostheses (3·5 [2·5-4·7]) were associated with a higher risk of revision for prosthetic joint infection. However, uncemented total, patellofemoral, or unicondylar knee replacement (RR for uncemented vs cemented total knee replacement 0·7 [95% CI 0·6-0·8], RR for patellofemoral vs cemented total knee replacement 0·3 [0·2-0·5], and RR for unicondylar vs cemented total knee replacement 0·5 [0·5-0·6]) were associated with lower risk of revision for prosthetic joint infection. Most of these factors had time-specific effects, depending on the time period post-surgery.
We have identified several risk factors for revision for prosthetic joint infection following knee replacement. Some of these factors are modifiable, and the use of targeted interventions or strategies could lead to a reduced risk of revision for prosthetic joint infection. Non-modifiable factors and the time-specific nature of the effects we have observed will allow clinicians to appropriately counsel patients preoperatively and tailor follow-up regimens.
National Institute for Health Research.
人工关节感染是膝关节置换术后的一种严重并发症。发生人工关节感染的风险受患者、手术和医疗保健系统因素的影响。现有证据受研究人群异质性、随访时间短、统计效能不足的限制,且未区分与干预措施相关的早期人工关节感染和更可能因血源性细菌播散引起的晚期感染。我们旨在评估这些因素与初次膝关节置换术后因人工关节感染而需返修的总体和特定时间相关性。
在这项队列研究中,我们分析了 2003 年至 2013 年间在英格兰和威尔士进行的初次膝关节置换术,以及 2003 年至 2014 年间因人工关节感染而进行的后续翻修手术。数据来自英国国家关节登记处与英格兰医院事件统计数据和威尔士患者发病数据库的关联。每一次初次置换都至少随访 12 个月,直到观察期结束(2014 年 12 月 31 日)或直到因人工关节感染、因其他原因、或因死亡而进行返修(以先发生者为准)。我们使用泊松和分段指数多水平模型来分析数据,以评估患者、手术和医疗保健系统因素与因人工关节感染而返修的风险之间的相关性。
在 2003 年至 2013 年间在英格兰和威尔士进行的 679010 次初次膝关节置换术中,有 3659 次在 2003 年至 2014 年间因人工关节感染而进行了后续翻修手术,中位随访时间为 4.6 年(IQR 2.6-6.9)。男性(与女性患者相比,男性的发生率比[RR]为 1.8 [95%CI 1.7-2.0])、年龄较小(年龄≥80 岁与<60 岁相比 RR 为 0.5 [0.4-0.6])、美国麻醉医师协会(ASA)分级较高(ASA 分级 3-5 与 1 级相比 RR 为 1.8 [1.6-2.1])、身体质量指数(BMI)较高(BMI≥30 kg/m2 与<25 kg/m2 相比 RR 为 1.5 [1.3-1.6])、慢性肺部疾病(RR 为 1.2 [1.1-1.3])、糖尿病(RR 为 1.4 [1.2-1.5])、肝脏疾病(RR 为 2.2 [1.6-2.9])、结缔组织和风湿性疾病(RR 为 1.5 [1.3-1.7])、外周血管疾病(RR 为 1.4 [1.1-1.7])、创伤手术(RR 为 1.9 [1.4-2.6])、既往化脓性关节炎(RR 为 4.9 [2.7-7.6])或炎性关节炎(RR 为 1.4 [1.2-1.7])、全身麻醉下手术(RR 为 1.1 [1.0-1.2])、胫骨骨移植(RR 为 2.0 [1.3-2.7])、使用后稳定固定轴承假体(RR 为后稳定固定轴承假体与非约束性固定轴承假体相比 1.4 [1.3-1.5])或约束性髁假体(RR 为 3.5 [2.5-4.7])与人工关节感染的返修风险较高相关。然而,非骨水泥全膝关节、髌股关节或单髁膝关节置换术(与骨水泥全膝关节置换术相比,非骨水泥全膝关节置换术 RR 为 0.7 [95%CI 0.6-0.8],髌股关节置换术 RR 为 0.3 [0.2-0.5],单髁膝关节置换术 RR 为 0.5 [0.5-0.6])与人工关节感染的返修风险较低相关。这些因素中的大多数都具有特定时间的效应,取决于术后的时间。
我们已经确定了膝关节置换术后因人工关节感染而需返修的几个风险因素。其中一些因素是可以改变的,针对这些因素实施靶向干预或策略可能会降低人工关节感染的返修风险。我们观察到的不可改变因素和特定时间效应,将使临床医生能够在术前适当地对患者进行咨询,并调整随访方案。
英国国家卫生研究院。