Laboratory of Nutrition, Faculty of Pharmacy, University Louis Pasteur, F-67401 Strasbourg, France.
Nutrients. 2019 Apr 21;11(4):895. doi: 10.3390/nu11040895.
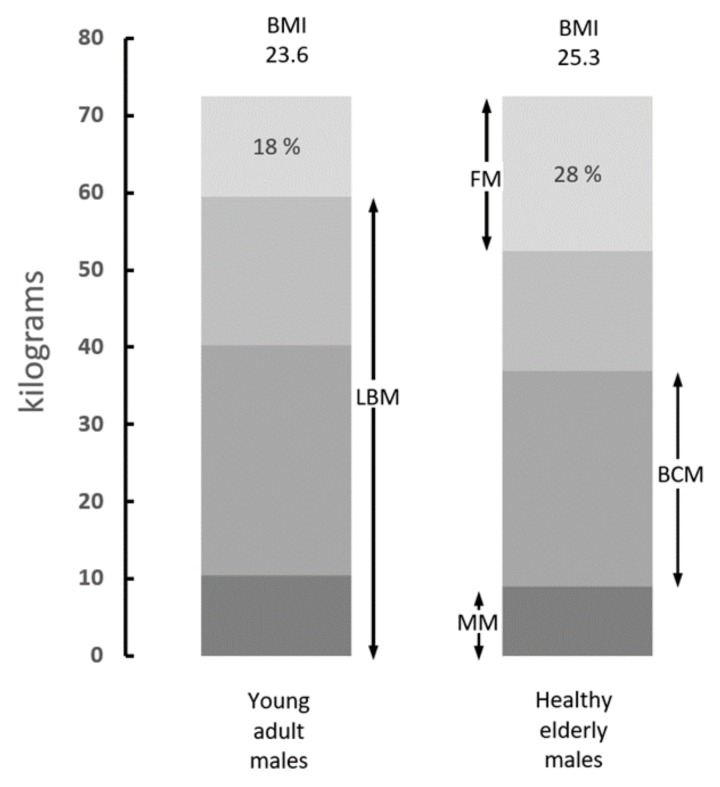
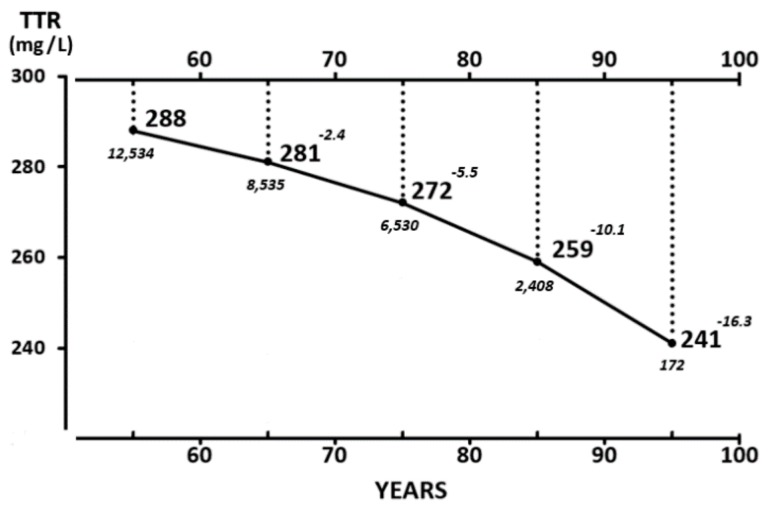
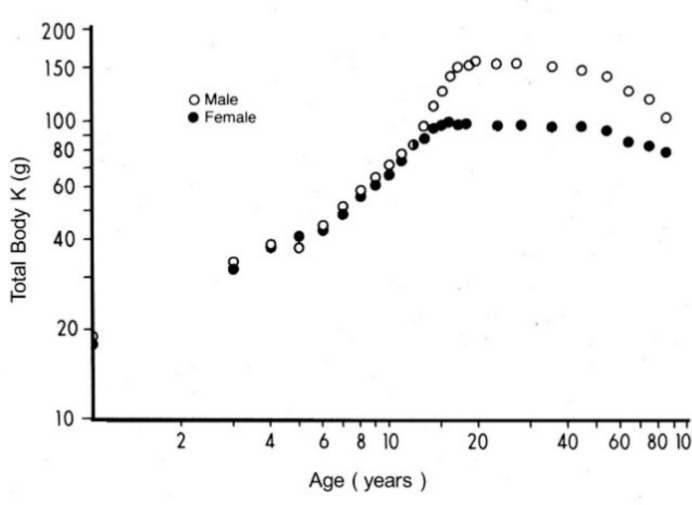
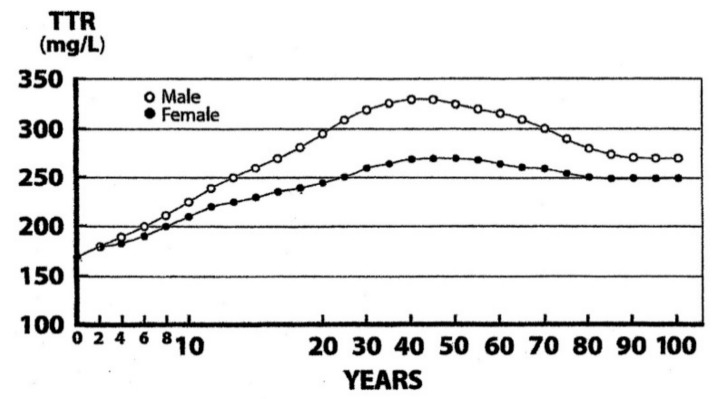
Skeletal muscle (SM) mass, the chief component of the structural compartment belonging to lean body mass (LBM), undergoes sarcopenia with increasing age. Decreased SM in elderly persons is a naturally occurring process that may be accelerated by acute or chronic nutritional deficiencies and/or inflammatory disorders, declining processes associated with harmful complications. A recently published position paper by European experts has provided an overall survey on the definition and diagnosis of sarcopenia in elderly persons. The present review describes the additional contributory role played by the noninvasive transthyretin (TTR) micromethod. The body mass index (BMI) formula is currently used in clinical studies as a criterion of good health to detect, prevent, and follow up on the downward trend of muscle mass. The recent upsurge of sarcopenic obesity with its multiple subclasses has led to a confused stratification of SM and fat stores, prompting workers to eliminate BMI from screening programs. As a result, investigators are now focusing on indices of protein status that participate in SM growth, maturation, and catabolism that might serve to identify sarcopenia trajectories. Plasma TTR is clearly superior to all other hepatic biomarkers, showing the same evolutionary patterns as those displayed in health and disease by both visceral and structural LBM compartments. As a result, this TTR parameter maintains positive correlations with muscle mass downsizing in elderly persons. The liver synthesis of TTR is downregulated in protein-depleted states and suppressed in cytokine-induced inflammatory disorders. TTR integrates the centrally-mediated regulatory mechanisms governing the balance between protein accretion and protein breakdown, emerging as the ultimate indicator of LBM resources. This review proposes the adoption of a gray zone defined by cut-off values ranging from 200 mg/L to 100 mg/L between which TTR plasma values may fluctuate and predict either the best or the worst outcome. The best outcome occurs when appropriate dietary, medicinal and surgical decisions are undertaken, resuming TTR synthesis which manifests rising trends towards pre-stress levels. The worst occurs when all therapeutic means fail to succeed, leading inevitably to complete exhaustion of LBM and SM metabolic resources with an ensuing fatal outcome. Some patients may remain unresponsive in the middle of the gray area, combining steady clinical states with persistent stagnant TTR values. Using the serial measurement of plasma TTR values, these last patients should be treated with the most aggressive and appropriate therapeutic strategies to ensure the best outcome.
骨骼肌(SM)质量是属于去脂体重(LBM)的结构性成分的主要组成部分,随着年龄的增长会发生肌肉减少症。老年人的 SM 减少是一种自然发生的过程,可能会因急性或慢性营养缺乏和/或炎症性疾病而加速,这些疾病与有害并发症相关的过程会下降。最近,欧洲专家发表了一份立场文件,对老年人肌肉减少症的定义和诊断进行了全面调查。本综述描述了非侵入性转甲状腺素蛋白(TTR)微量法的额外贡献作用。目前,在临床研究中,体质指数(BMI)公式被用作健康的标准,用于检测、预防和跟踪肌肉质量的下降趋势。最近,由于多种亚类的肌少症肥胖的出现,导致了 SM 和脂肪储存的混乱分层,促使研究人员从筛查计划中删除 BMI。因此,研究人员现在专注于参与 SM 生长、成熟和分解代谢的蛋白质状态指标,这些指标可能有助于识别肌肉减少症轨迹。血浆 TTR 明显优于所有其他肝生物标志物,其显示的进化模式与内脏和结构性 LBM 区室在健康和疾病中的模式相同。因此,该 TTR 参数与老年人的肌肉质量缩小呈正相关。在蛋白质缺乏状态下,肝脏合成 TTR 会下调,在细胞因子诱导的炎症性疾病中会受到抑制。TTR 整合了中枢介导的调节机制,控制着蛋白质积累和蛋白质分解之间的平衡,是 LBM 资源的最终指标。本综述提出采用介于 200mg/L 至 100mg/L 之间的截值定义的灰色区域,在此范围内,TTR 血浆值可能会波动,并预测最佳或最差结果。最佳结果发生在采取适当的饮食、药物和手术决策时,恢复 TTR 合成,表现出向应激前水平上升的趋势。最差结果发生在所有治疗方法都失败时,不可避免地导致 LBM 和 SM 代谢资源完全耗尽,随之而来的是致命的结果。一些患者可能处于灰色区域的中间,处于稳定的临床状态,同时 TTR 值持续停滞。通过连续测量血浆 TTR 值,应对这些患者采用最积极和适当的治疗策略,以确保最佳结果。