Paris Translational Research Center for Organ Transplantation, Institut National de la Santé et de la Recherche Médicale, Unité Mixte de Recherche-S970, Paris, France.
Department of Nephrology and Organ Transplantation, Saint-Louis Hospital, Assistance Publique-Hôpitaux de Paris, Institut National de la Santé et de la Recherche Médicale, Unité U1160, Paris, France.
Am J Transplant. 2019 Oct;19(10):2865-2875. doi: 10.1111/ajt.15397. Epub 2019 May 24.
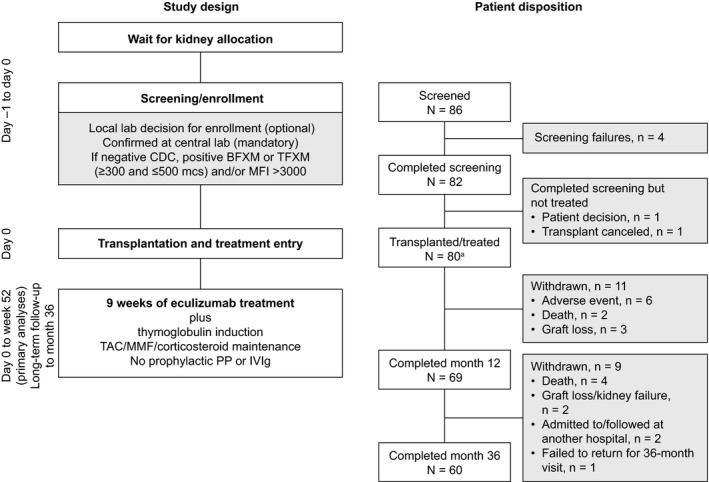
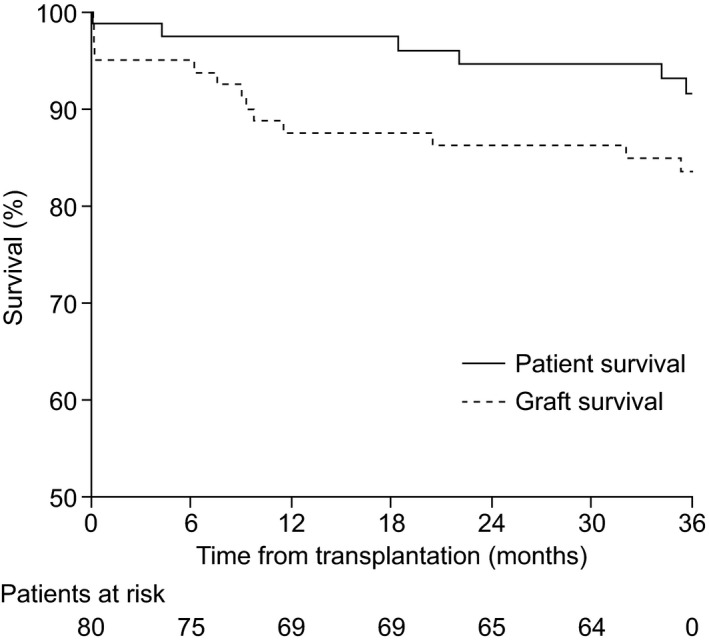
The presence of preformed donor-specific antibodies in transplant recipients increases the risk of acute antibody-mediated rejection (AMR). Results of an open-label single-arm trial to evaluate the safety and efficacy of eculizumab in preventing acute AMR in recipients of deceased-donor kidney transplants with preformed donor-specific antibodies are reported. Participants received eculizumab as follows: 1200 mg immediately before reperfusion; 900 mg on posttransplant days 1, 7, 14, 21, and 28; and 1200 mg at weeks 5, 7, and 9. All patients received thymoglobulin induction therapy and standard maintenance immunosuppression including steroids. The primary end point was treatment failure rate, a composite of biopsy-proved grade II/III AMR (Banff 2007 criteria), graft loss, death, or loss to follow-up, within 9 weeks posttransplant. Eighty patients received transplants (48 women); the median age was 52 years (range 24-70 years). Observed treatment failure rate (8.8%) was significantly lower than expected for standard care (40%; P < .001). By 9 weeks, 3 of 80 patients had experienced AMR, and 4 of 80 had experienced graft loss. At 36 months, graft and patient survival rates were 83.4% and 91.5%, respectively. Eculizumab was well tolerated and no new safety concerns were identified. Eculizumab has the potential to provide prophylaxis against injury caused by acute AMR in such patients (EudraCT 2010-019631-35).
移植受者体内预先存在的供体特异性抗体增加了急性抗体介导的排斥反应(AMR)的风险。报告了一项开放标签单臂试验的结果,该试验评估了依库珠单抗在预防预先存在供体特异性抗体的已故供体肾移植受者中急性 AMR 的安全性和有效性。参与者接受依库珠单抗的方案如下:再灌注前立即给予 1200mg;移植后第 1、7、14、21 和 28 天给予 900mg;第 5、7 和 9 周给予 1200mg。所有患者均接受了胸腺球蛋白诱导治疗和包括类固醇在内的标准维持免疫抑制治疗。主要终点是 9 周内移植后活检证实的 II/III 级 AMR(Banff 2007 标准)、移植物丢失、死亡或失访的治疗失败率。80 例患者接受了移植(48 例女性);中位年龄为 52 岁(范围 24-70 岁)。观察到的治疗失败率(8.8%)明显低于标准治疗(40%;P<0.001)。在 9 周时,80 例患者中有 3 例发生 AMR,80 例中有 4 例发生移植物丢失。在 36 个月时,移植物和患者的存活率分别为 83.4%和 91.5%。依库珠单抗耐受性良好,未发现新的安全问题。依库珠单抗有可能预防此类患者急性 AMR 引起的损伤(EudraCT 2010-019631-35)。