Wu Di, Chen Tiejun, Jiang Han, Duan Chongyang, Zhang Xinjian, Lin Yiguang, Chen Size, Wu Fenfang
Department of Central Laboratory, Shenzhen Hospital, Beijing University of Chinese Medicine, Shenzhen, China.
Department of Oncology, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, China.
J Oncol. 2019 Mar 19;2019:3406972. doi: 10.1155/2019/3406972. eCollection 2019.
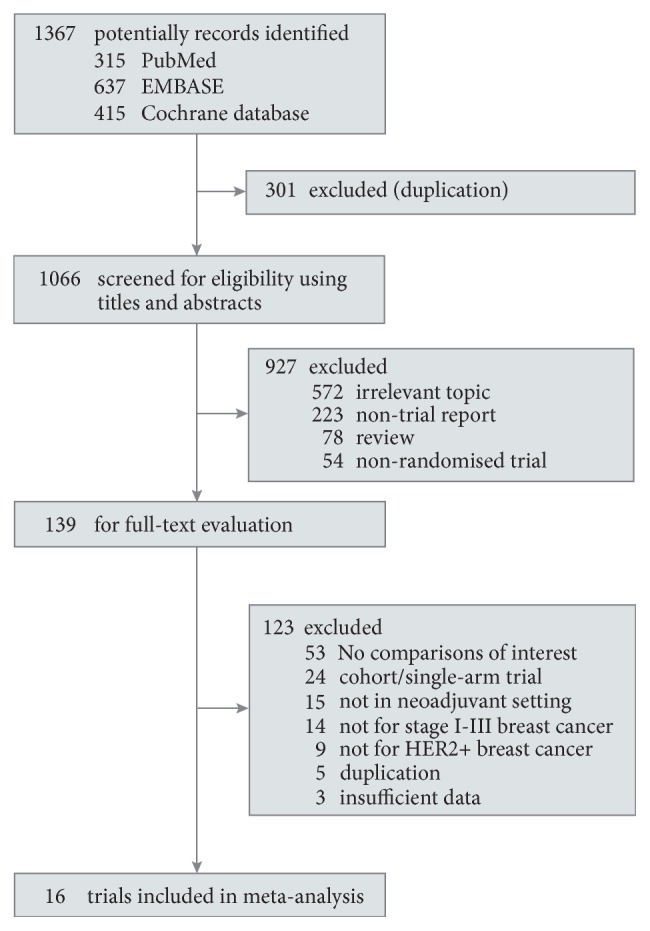
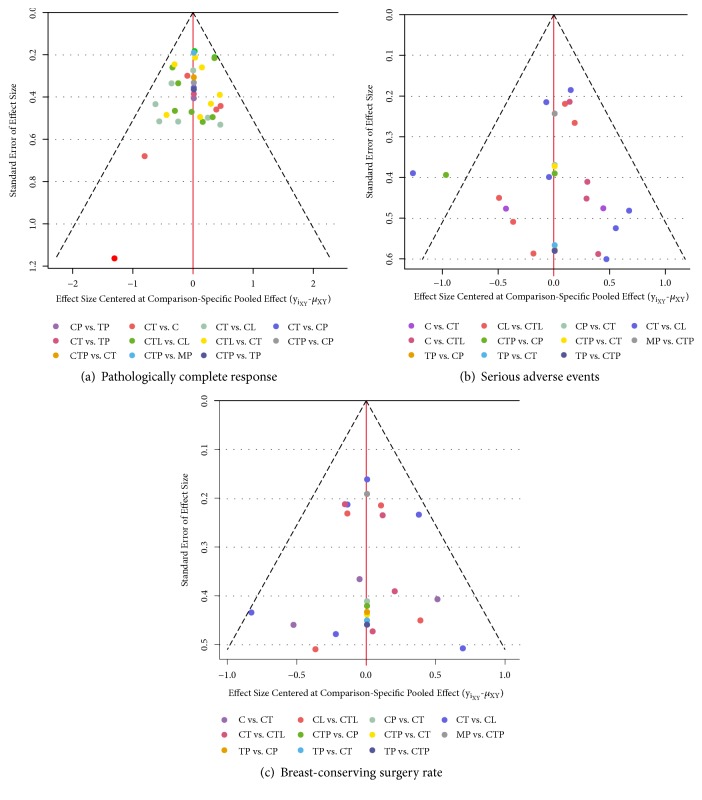
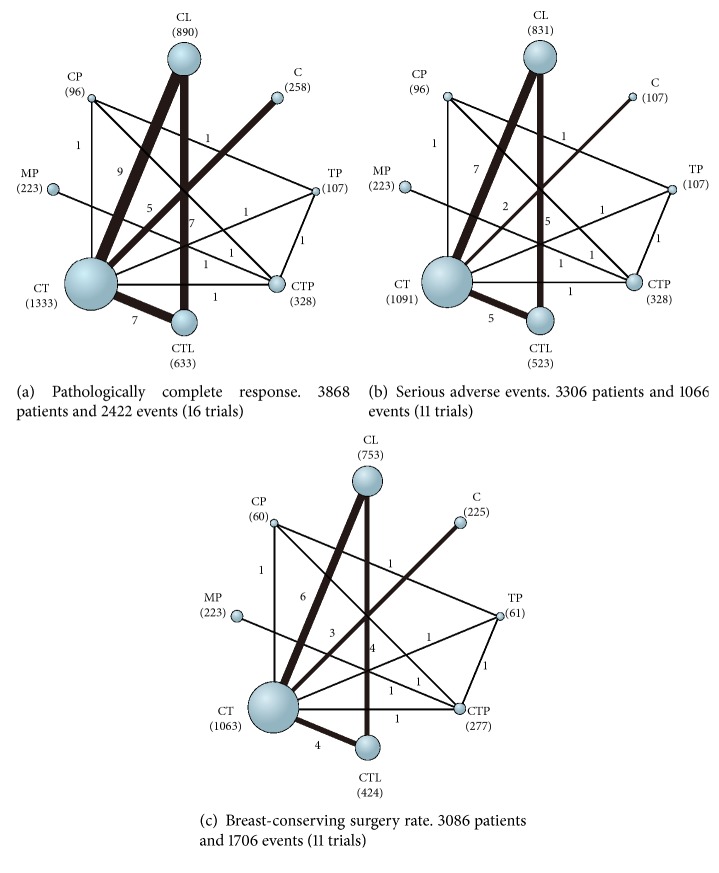
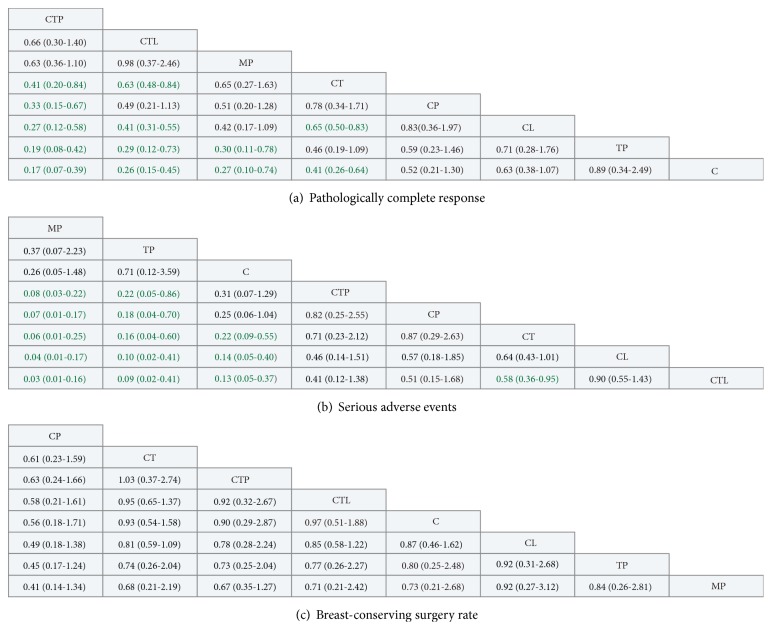
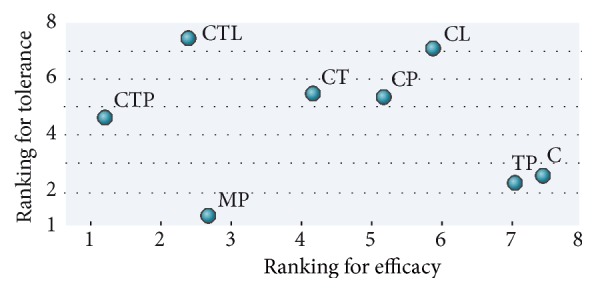
This network meta-analysis addresses the need for evidence-based best-practice treatment regimens for HER2-positive breast cancer. We compared the relative efficacy and tolerability of currently available HER2-positive neoadjuvant immunotherapy regimens based on systematic searches of available randomized controlled trials (RCTs) data. Based on intention-to-treat principle, pathological complete response (pCR), overall serious adverse events (SAEs), and breast-conserving surgery (BCS) rate were analyzed using random-effect, Bayesian network meta-analysis, and standard pairwise meta-analysis. 16 RCTs (3868 patients) were included. Analyzed treatment regimens were as follows: chemotherapy+trastuzumab+pertuzumab (CTP), trastuzumab emtansine+pertuzumab (MP), chemotherapy+trastuzumab (CT), chemotherapy+pertuzumab (CP), trastuzumab+pertuzumab (TP), chemotherapy+trastuzumab+lapatinib (CTL), and chemotherapy+lapatinib (CL), and chemotherapy (C) alone. We found that, for the chance of achieving pCR, CTP was ranked first (SUCRA: 97%), followed by CTL, MP, and CT (SUCRA: 80%, 75%, and 55%, resp.). MP provided the safest regimen (SUCRA: 97%), then TP, C, and TPC (SUCRA: 82%, 76%, and 47%, resp.). CTL proved the most toxic therapy (SUCRA: 7%). No significant difference between neoadjuvant regimens was identified for BCS. Hormone receptor status did not impact ORs for pCR in any regimen. In conclusion, our findings support CTP as the optimum neoadjuvant regimen for HER2-positive breast cancer, with the best pCR and acceptable toxicity compared with CT. MP provides a therapeutic option for patients with poor performance status.
这项网络荟萃分析满足了对HER2阳性乳腺癌基于循证的最佳治疗方案的需求。我们通过系统检索现有随机对照试验(RCT)数据,比较了目前可用的HER2阳性新辅助免疫治疗方案的相对疗效和耐受性。基于意向性治疗原则,使用随机效应、贝叶斯网络荟萃分析和标准成对荟萃分析对病理完全缓解(pCR)、总体严重不良事件(SAE)和保乳手术(BCS)率进行分析。纳入了16项RCT(3868例患者)。分析的治疗方案如下:化疗+曲妥珠单抗+帕妥珠单抗(CTP)、曲妥珠单抗恩美曲妥珠单抗+帕妥珠单抗(MP)、化疗+曲妥珠单抗(CT)、化疗+帕妥珠单抗(CP)、曲妥珠单抗+帕妥珠单抗(TP)、化疗+曲妥珠单抗+拉帕替尼(CTL)、化疗+拉帕替尼(CL)以及单纯化疗(C)。我们发现,就实现pCR的可能性而言,CTP排名第一(累积排序曲线下面积:97%),其次是CTL、MP和CT(累积排序曲线下面积分别为80%、75% 和55%)。MP提供了最安全的方案(累积排序曲线下面积:97%),其次是TP、C和TPC(累积排序曲线下面积分别为82%、76% 和47%)。CTL被证明是毒性最大的治疗方法(累积排序曲线下面积:7%)。新辅助治疗方案在BCS方面未发现显著差异。激素受体状态对任何治疗方案的pCR的比值比均无影响。总之,我们的研究结果支持CTP作为HER2阳性乳腺癌的最佳新辅助治疗方案,与CT相比,其pCR最佳且毒性可接受。MP为身体状况较差的患者提供了一种治疗选择。