Department of Respiratory Medicine, Quanzhou First Hospital, Quanzhou, China.
Department of Lung Cancer and Immunology, Shanghai Pulmonary Hospital, Tongji University, Shanghai, China.
Cancer Med. 2019 Jun;8(6):2858-2866. doi: 10.1002/cam4.2183. Epub 2019 Apr 24.
Although oncogenic driver mutations were thought to be mutually exclusive in non-small cell lung cancer (NSCLC), certain tumors harbor co-occurring mutations and represent a rare molecular subtype. The evaluation of the clinical features and therapeutic response associated with this NSCLC subtype will be vital for understanding the heterogeneity of treatment response and improving the management of these patients.
This retrospective study included 3774 samples from patients diagnosed with NSCLC. All samples were screened for EGFR, ALK, ROS1, KRAS, and BRAF mutation using the amplification-refractory mutation system. The relationship between concomitant driver mutations and clinicopathologic characteristics, and patient clinical outcomes were evaluated.
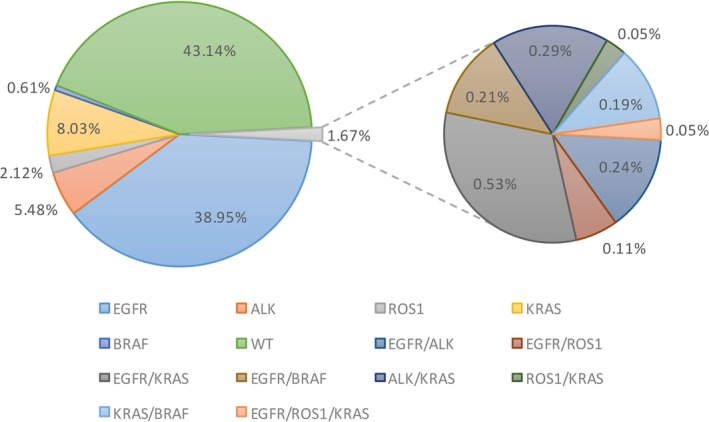
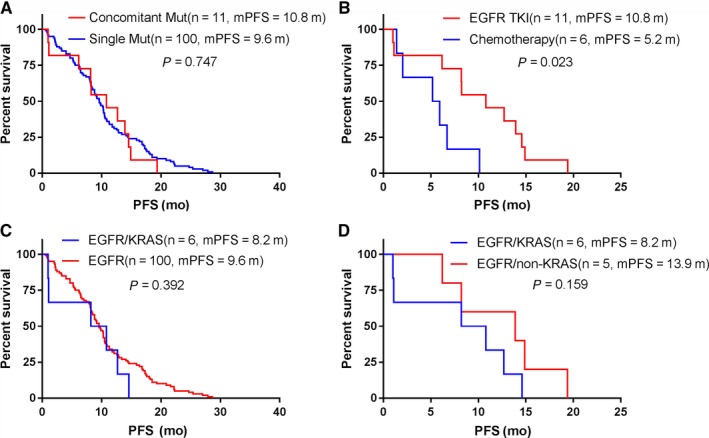
Sixty-three (1.7%) samples had more than one driver gene mutation. Among these, 43 were coalterations with an EGFR mutation, 20 with an ALK rearrangement, and eight with an ROS1 rearrangement. Except for ROS1 concomitant mutations that were more frequent in male patients (87.5%, P = 0.020), the clinicopathological features of the concomitant mutation patients were not significantly different from those harboring a single EGFR, ALK, or ROS1 mutation. Furthermore, first-line EGFR-TKI treatment did not significantly improve the progression-free survival (PFS) of patients harboring EGFR concomitant mutation, compared to patients harboring a single EGFR mutation. However, for EGFR concomitant mutation patients, TKI therapy was more effective than chemotherapy (median PFS of 10.8 vs 5.2 months, P = 0.023). Lastly, KRAS mutations did not influence the EGFR-TKI therapy treatment effect.
In this study, concomitant mutations were found in 1.7% of the NSCLC. EGFR-TKI therapy was more effective than chemotherapy for patients harboring EGFR concomitant mutation, and ROS1 concomitant mutations were more frequent in male patients. For patients harboring coalterations with an ALK or ROS1 rearrangement, we should be cautious when considering the therapeutic options.
虽然非小细胞肺癌(NSCLC)中的致癌驱动基因突变被认为是相互排斥的,但某些肿瘤存在共发生突变,代表一种罕见的分子亚型。评估与这种 NSCLC 亚型相关的临床特征和治疗反应对于理解治疗反应的异质性和改善这些患者的管理至关重要。
本回顾性研究纳入了 3774 例 NSCLC 患者的样本。所有样本均采用扩增受阻突变系统(amplification-refractory mutation system)检测 EGFR、ALK、ROS1、KRAS 和 BRAF 突变。评估了伴随驱动基因突变与临床病理特征以及患者临床结局的关系。
63 例(1.7%)样本存在两种以上的驱动基因突变。其中,43 例与 EGFR 突变共存,20 例与 ALK 重排共存,8 例与 ROS1 重排共存。除了 ROS1 共突变在男性患者中更为常见(87.5%,P=0.020)外,共突变患者的临床病理特征与单独存在 EGFR、ALK 或 ROS1 突变的患者无显著差异。此外,与单独存在 EGFR 突变的患者相比,一线 EGFR-TKI 治疗并未显著改善 EGFR 共突变患者的无进展生存期(progression-free survival,PFS)。然而,对于 EGFR 共突变患者,TKI 治疗比化疗更有效(中位 PFS 分别为 10.8 个月和 5.2 个月,P=0.023)。最后,KRAS 突变并不影响 EGFR-TKI 治疗效果。
在本研究中,NSCLC 中发现了 1.7%的共突变。与单独存在 EGFR 突变的患者相比,EGFR-TKI 治疗对存在 EGFR 共突变的患者更有效,且 ROS1 共突变在男性患者中更为常见。对于存在 ALK 或 ROS1 重排共突变的患者,在考虑治疗选择时应谨慎。