Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Department of Pediatrics, McMaster University Medical Center, Hamilton, ON, Canada.
Front Immunol. 2019 Apr 9;10:745. doi: 10.3389/fimmu.2019.00745. eCollection 2019.
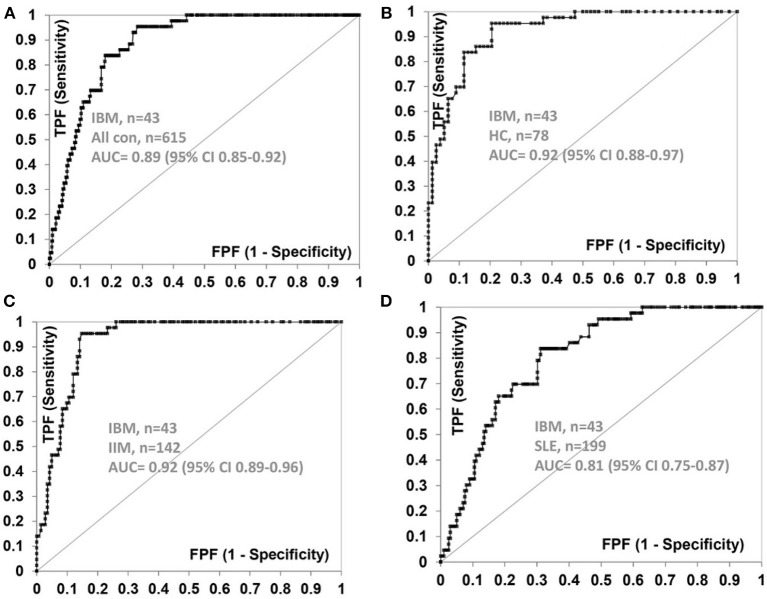
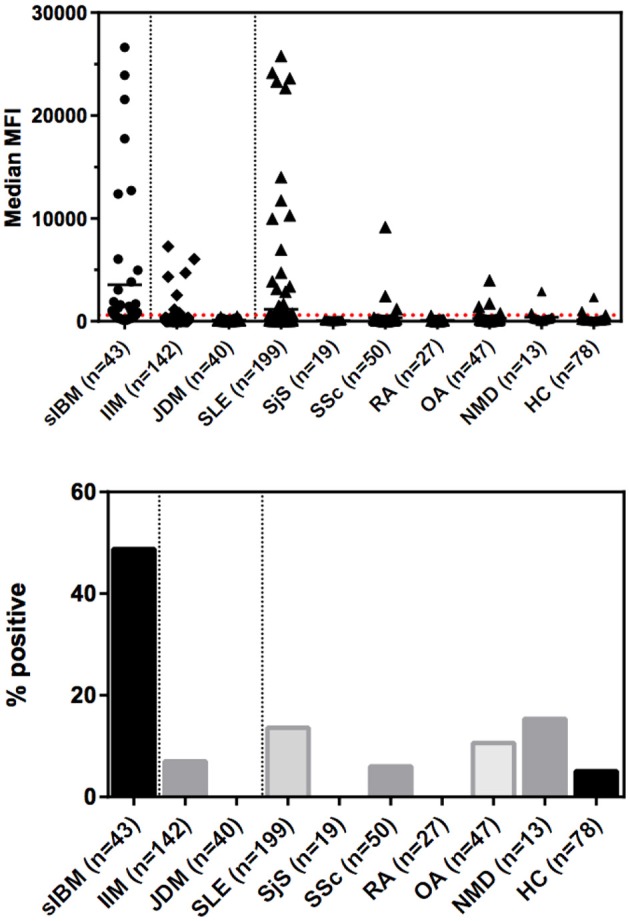
Sporadic Inclusion Body Myositis (sIBM) is an inflammatory myopathy (IIM) without a specific diagnostic biomarker until autoantibodies to the cytosolic 5'-nucleotidase 1A (/Mup44) were reported. The objectives of our study were to determine the sensitivity and specificity of anti-NT5c1A for sIBM, demonstrate demographic, clinical and serological predictors for anti-NT5c1A positivity and determine if anti-nuclear antibody (ANA) indirect immunofluorescence (IIF) staining on HEp-2 cells is a reliable screening method for anti-NT5c1A. Sera from sIBM patients and controls were stored at -80°C until required for analysis. IgG antibodies to NT5c1A were detected by an addressable laser bead immunoassay (ALBIA) using a full-length human recombinant protein. Autoantibodies to other autoimmune myopathy antigens (Jo-1, OJ, TIF1y, PL-12, SAE, EJ, MDA5, PL7, SRP, NXP2, MI-2) were detected by line immunoassay (LIA), chemiluminescence immunoassay (CIA) or enzyme linked immunosorbent assay (ELISA) and ANA detected by IIF on HEp-2 substrate. Demographic, clinical and serological data were obtained by chart review. Forty-three patients with sIBM, 537 disease control patients with other autoimmune, degenerative and neuromuscular diseases, and 78 healthy controls were included. 48.8% (21/43) of sIBM patients were positive for anti-NT5c1A. The overall sensitivity, specificity, positive predictive value, and negative predictive value of anti-NT5c1A for sIBM were 0.49, 0.92, 0.29, and 0.96, respectively. Compared to sIBM, the frequency of anti-NT5c1A was lower in both the disease control group (8.8%, OR 0.10 [95%CI: 0.05-0.20], < 0.0001) and in the apparently healthy control group (5.1%, OR 0.06 [95%CI: 0.02-0.18], < 0.0001). In the univariable analysis, sIBM patients with more severe muscle weakness were more likely to be anti-NT5c1A positive (OR 4.10 [95% CI: 1.17, 14.33], = 0.027), although this was not statistically significant (adjusted OR 4.30 [95% CI: 0.89, 20.76], = 0.069) in the multivariable analysis. The ANA of sIBM sera did not demonstrate a consistent IIF pattern associated with anti-NT5c1A. Anti-NT5c1A has moderate sensitivity and high specificity for sIBM using ALBIA. The presence of anti-NT5c1A antibodies may be associated with muscle weakness. Anti-NT5c1A antibodies were not associated with a specific IIF staining pattern, hence screening using HEp-2 substrate is unlikely to be a useful predictor for presence of these autoantibodies.
散发性包涵体肌炎(sIBM)是一种炎症性肌病(IIM),直到细胞溶质 5'-核苷酸酶 1A(/Mup44)的自身抗体被报道之前,都没有特定的诊断生物标志物。我们研究的目的是确定抗-NT5c1A 对 sIBM 的敏感性和特异性,证明抗-NT5c1A 阳性的人口统计学、临床和血清学预测因素,并确定抗核抗体(ANA)间接免疫荧光(IIF)染色在 HEp-2 细胞上是否是抗-NT5c1A 的可靠筛选方法。sIBM 患者和对照者的血清在需要分析时在-80°C 下储存。使用全长人重组蛋白通过可寻址激光珠免疫测定(ALBIA)检测针对 NT5c1A 的 IgG 抗体。使用线免疫测定(LIA)、化学发光免疫测定(CIA)或酶联免疫吸附测定(ELISA)检测针对其他自身免疫性肌病抗原(Jo-1、OJ、TIF1y、PL-12、SAE、EJ、MDA5、PL7、SRP、NXP2、MI-2)的自身抗体,并使用 HEp-2 底物进行 IIF 检测 ANA。通过图表审查获得人口统计学、临床和血清学数据。纳入了 43 名 sIBM 患者、537 名患有其他自身免疫性、退行性和神经肌肉疾病的疾病对照患者和 78 名健康对照者。48.8%(21/43)的 sIBM 患者抗-NT5c1A 阳性。抗-NT5c1A 对 sIBM 的总体敏感性、特异性、阳性预测值和阴性预测值分别为 0.49、0.92、0.29 和 0.96。与 sIBM 相比,疾病对照组(8.8%,OR 0.10 [95%CI:0.05-0.20],<0.0001)和明显健康对照组(5.1%,OR 0.06 [95%CI:0.02-0.18],<0.0001)中抗-NT5c1A 的频率较低。在单变量分析中,肌肉无力更严重的 sIBM 患者更有可能为抗-NT5c1A 阳性(OR 4.10 [95%CI:1.17,14.33],=0.027),尽管在多变量分析中这并不具有统计学意义(调整后的 OR 4.30 [95%CI:0.89,20.76],=0.069)。sIBM 血清中的 ANA 没有显示出与抗-NT5c1A 相关的一致 IIF 模式。ALBIA 对 sIBM 具有中等敏感性和高度特异性的抗-NT5c1A。抗-NT5c1A 抗体的存在可能与肌肉无力有关。抗-NT5c1A 抗体与特定的 IIF 染色模式无关,因此使用 HEp-2 底物进行筛查不太可能成为存在这些自身抗体的有用预测指标。