Ma Ka Wing, She Wong Hoi, Chan Albert Chi Yan, Cheung Tan To, Fung James Yan Yue, Dai Wing Chiu, Lo Chung Mau, Chok Kenneth Siu Ho
Department of Surgery, the University of Hong Kong, Hong Kong, China.
Department of Surgery and State Key Laboratory for Liver Research, the University of Hong Kong, 102 Pokfulam Road, Hong Kong, China.
World J Gastrointest Oncol. 2019 Apr 15;11(4):322-334. doi: 10.4251/wjgo.v11.i4.322.
Liver transplantation (LT) is regarded as the best treatment for both primary and recurrent hepatocellular carcinoma (HCC). Post-transplant HCC recurrence rate is relatively low but significant, ranging from 10%-30% according to different series. When recurrence happens, it is usually extrahepatic and associated with poor prognosis. A predictive model that allows patient stratification according to recurrence risk can help to individualize post-transplant surveillance protocol and guidance of the use of anti-tumor immunosuppressive agents.
To develop a scoring system to predict HCC recurrence after LT in an Asian population.
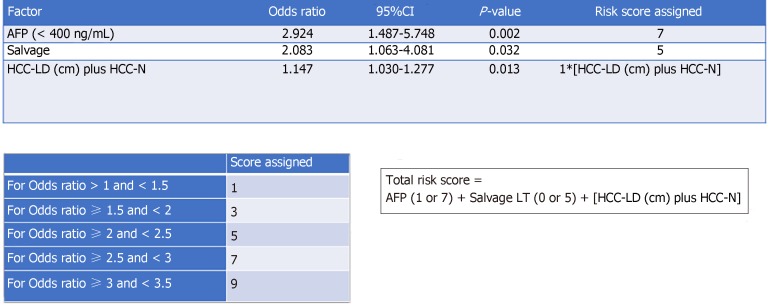
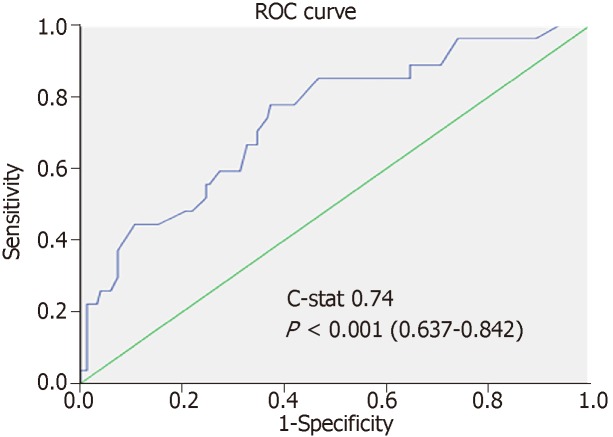
Consecutive patients having LT for HCC from 1995 to 2016 at our hospital were recruited. They were randomized into the training set and the validation set in a 60:40 ratio. Multivariable Cox regression model was used to identity factors associated with HCC recurrence. A risk score was assigned to each factor according to the odds ratio. Accuracy of the score was assessed by the area under the receiver operating characteristic curve.
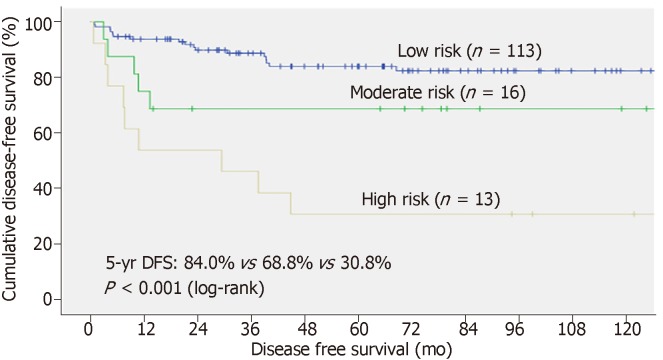
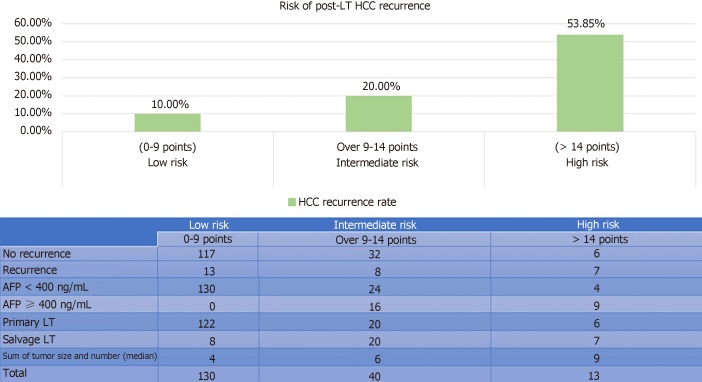
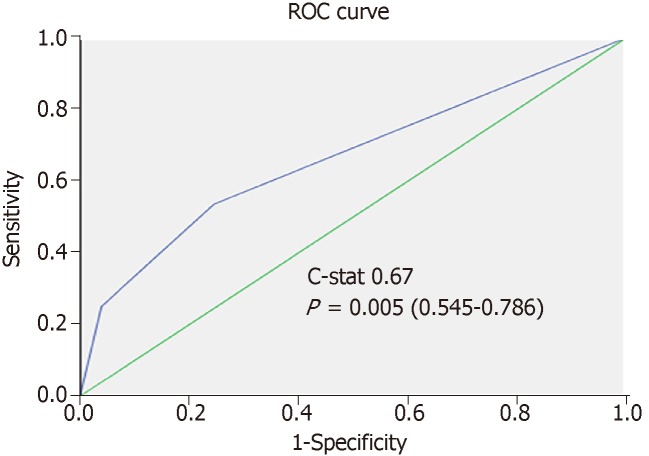
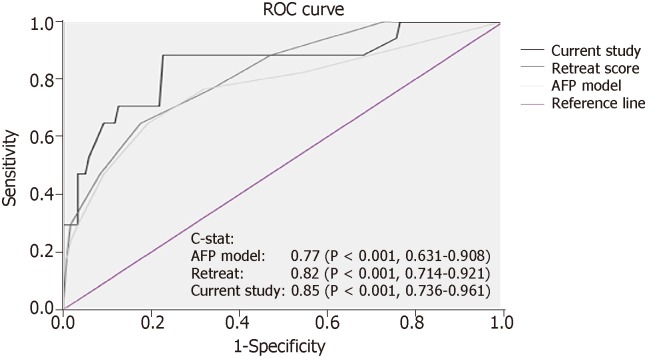
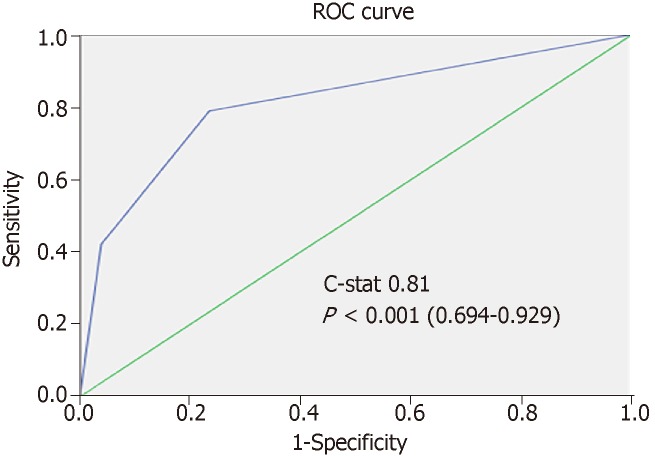
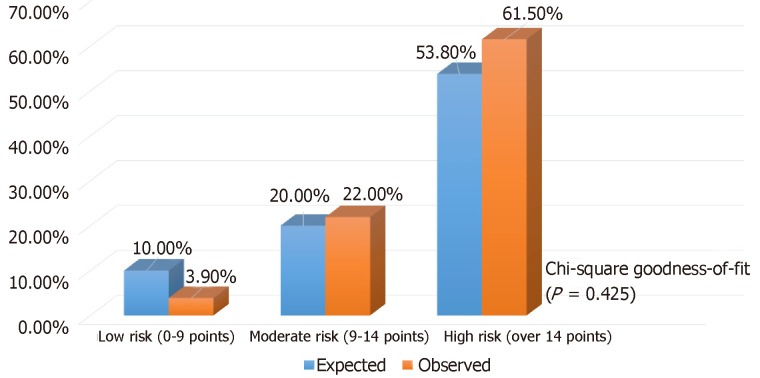
In total, 330 patients were eligible for analysis (183 in training and 147 in validation). Recurrent HCC developed in 14.2% of them. The median follow-up duration was 65.6 mo. The 5-year disease-free and overall survival rates were 78% and 80%, respectively. On multivariate analysis, alpha-fetoprotein > 400 ng/mL [ = 0.012, hazard ratio (HR) 2.92], sum of maximum tumor size and number ( = 0.013, HR 1.15), and salvage LT ( = 0.033, HR 2.08) were found to be independent factors for disease-free survival. A risk score was calculated for each patient with good discriminatory power (c-stat 0.748 and 0.85, respectively, in the training and validation sets). With the derived scores, patients were classified into low- (0-9), moderate- (> 9-14), and high-risk groups (> 14), and the risk of HCC recurrence in the training and validation sets was 10%, 20%, 54% (c-stat 0.67) and 4%, 22%, 62% (c-stat 0.811), accordingly. The risk stratification model was validated with chi-squared goodness-of-fit test ( = 0.425).
A validated predictive model featuring alpha-fetoprotein, salvage LT, and the sum of largest tumor diameter and total number of tumor nodule provides simple and reliable guidance for individualizing postoperative surveillance strategy.
肝移植(LT)被视为原发性和复发性肝细胞癌(HCC)的最佳治疗方法。移植后HCC复发率相对较低但仍较为显著,根据不同系列报道,复发率在10% - 30%之间。当复发发生时,通常为肝外复发且预后较差。一个能够根据复发风险对患者进行分层的预测模型有助于使移植后监测方案个体化,并指导抗肿瘤免疫抑制剂的使用。
建立一个评分系统以预测亚洲人群肝移植后HCC的复发情况。
纳入1995年至2016年在我院因HCC接受肝移植的连续患者。他们以60:40的比例随机分为训练集和验证集。采用多变量Cox回归模型来确定与HCC复发相关的因素。根据比值比为每个因素分配一个风险评分。通过受试者操作特征曲线下面积评估评分的准确性。
总共330例患者符合分析条件(训练集183例,验证集147例)。其中14.2%发生了复发性HCC。中位随访时间为65.6个月。5年无病生存率和总生存率分别为78%和80%。多因素分析显示,甲胎蛋白>400 ng/mL(P = 0.012,风险比[HR] 2.92)、最大肿瘤大小与数量之和(P = 0.013,HR 1.15)以及挽救性肝移植(P = 0.033,HR 2.08)是无病生存的独立因素。为每位患者计算了具有良好区分能力的风险评分(训练集和验证集的c统计量分别为0.748和0.85)。根据得出的评分,患者被分为低风险(0 - 9分)、中度风险(>9 - 14分)和高风险组(>14分),训练集和验证集中HCC复发风险分别为10%、20%、54%(c统计量0.67)和4%、22%、62%(c统计量0.811)。风险分层模型通过卡方拟合优度检验进行验证(P = 0.425)。
一个以甲胎蛋白、挽救性肝移植以及最大肿瘤直径与肿瘤结节总数之和为特征的经过验证的预测模型为个体化术后监测策略提供了简单可靠的指导。