Department of Statistics, USBE, Umeå University, Umeå, Sweden.
Paediatrics, Department of Clinical Sciences, Umeå University, SE-901 85, Umeå, Sweden.
Diabetologia. 2019 Jul;62(7):1173-1184. doi: 10.1007/s00125-019-4874-5. Epub 2019 Apr 30.
AIMS/HYPOTHESIS: Single-centre studies and meta-analyses have found diverging results as to which early life factors affect the risk of type 1 diabetes during childhood. We wanted to use a large, nationwide, prospective database to further clarify and analyse the associations between perinatal factors and the subsequent risk for childhood-onset type 1 diabetes using a case-control design.
The Swedish Childhood Diabetes Register was linked to the Swedish Medical Birth Register and National Patient Register, and 14,949 cases with type 1 diabetes onset at ages 0-14 years were compared with 55,712 matched controls born from the start of the Medical Birth Register in 1973 to 2013. After excluding confounders (i.e. children multiple births, those whose mother had maternal diabetes and those with a non-Nordic mother), we used conditional logistic regression analyses to determine risk factors for childhood-onset type 1 diabetes. We used WHO ICD codes for child and maternal diagnoses.
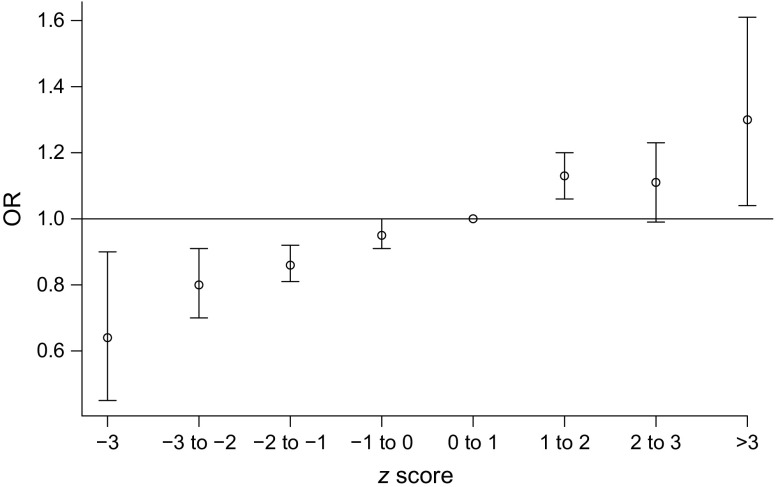
In multivariate analysis, there were small but statistically significant associations between higher birthweight z score (OR 1.08, 95% CI 1.06, 1.10), delivery by Caesarean section (OR 1.08, 95% CI 1.02, 1.15), premature rupture of membranes (OR 1.08, 95% CI 1.01, 1.16) and maternal urinary tract infection during pregnancy (OR 1.39, 95% CI 1.04, 1.86) and the subsequent risk of childhood-onset type 1 diabetes. Birth before 32 weeks of gestation was associated with a lower risk of childhood-onset type 1 diabetes compared with full-term infants (OR 0.54, 95% CI 0.38, 0.76), whereas birth between 32 and 36 weeks' gestation was associated with a higher risk (OR 1.24, 95% CI 1.14, 1.35). In subgroup analyses (birth years 1992-2013), maternal obesity was independently associated with subsequent type 1 diabetes in the children (OR 1.27, 95% CI 1.15, 1.41) and rendered the association with Caesarean section non-significant. In contrast to previous studies, we found no association of childhood-onset type 1 diabetes with maternal-child blood-group incompatibility, maternal pre-eclampsia, perinatal infections or treatment of the newborn with phototherapy for neonatal jaundice. The proportion of children with neonatal jaundice was significantly higher in the 1973-1982 birth cohort compared with later cohorts.
CONCLUSIONS/INTERPRETATION: Perinatal factors make small but statistically significant contributions to the overall risk of childhood-onset type 1 diabetes. Some of these risk factors, such as maternal obesity, may be amendable with improved antenatal care. Better perinatal practices may have affected some previously noted risk factors over time.
目的/假设:单中心研究和荟萃分析得出的结果存在差异,即哪些生命早期因素会影响儿童时期 1 型糖尿病的风险。我们希望使用一个大型的全国性前瞻性数据库,使用病例对照设计,进一步阐明和分析围产期因素与随后儿童期 1 型糖尿病风险之间的关系。
将瑞典儿童糖尿病登记处与瑞典医疗出生登记处和国家患者登记处相关联,并将 14949 例发病年龄在 0-14 岁的 1 型糖尿病病例与 55712 例出生于 1973 年至 2013 年医疗出生登记处开始的年龄匹配对照进行比较。在排除混杂因素(即多胎儿童、母亲患有糖尿病和母亲非北欧裔)后,我们使用条件逻辑回归分析来确定儿童期 1 型糖尿病的危险因素。我们使用世界卫生组织的儿童和母亲诊断 ICD 代码。
多变量分析显示,出生体重 z 评分较高(OR 1.08,95%CI 1.06,1.10)、剖宫产(OR 1.08,95%CI 1.02,1.15)、胎膜早破(OR 1.08,95%CI 1.01,1.16)和母亲妊娠期间尿路感染(OR 1.39,95%CI 1.04,1.86)与儿童期 1 型糖尿病的后续风险之间存在微小但具有统计学意义的关联。与足月婴儿相比,妊娠 32 周前出生与儿童期 1 型糖尿病的风险较低(OR 0.54,95%CI 0.38,0.76),而妊娠 32-36 周出生与风险较高相关(OR 1.24,95%CI 1.14,1.35)。在亚组分析(1992-2013 年出生年份)中,母亲肥胖与儿童随后发生 1 型糖尿病独立相关(OR 1.27,95%CI 1.15,1.41),并且使剖宫产的关联变得不显著。与以往的研究不同,我们没有发现儿童期 1 型糖尿病与母婴血型不合、母亲子痫前期、围产期感染或新生儿黄疸接受光疗治疗之间存在关联。与较晚的队列相比,1973-1982 年出生队列中新生儿黄疸的儿童比例明显更高。
结论/解释:围产期因素对儿童期 1 型糖尿病的总体风险有微小但具有统计学意义的贡献。一些风险因素,如母亲肥胖,可能可以通过改善产前护理来改善。随着时间的推移,更好的围产期实践可能会影响一些以前注意到的风险因素。