Kang Taewook, Park Si Young, Kang Chun Hyung, Lee Soon Hyuck, Park Jong Hoon, Suh Seung Woo
Department of Orthopaedics, Korea University College of Medicine, Seoul, Republic of Korea.
Medicine (Baltimore). 2019 May;98(18):e15451. doi: 10.1097/MD.0000000000015451.
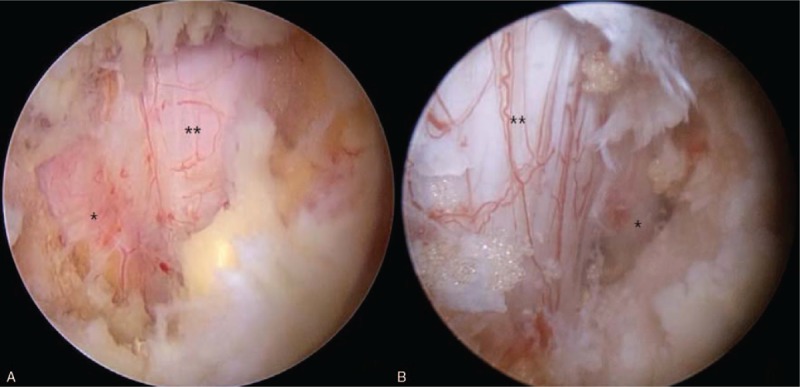
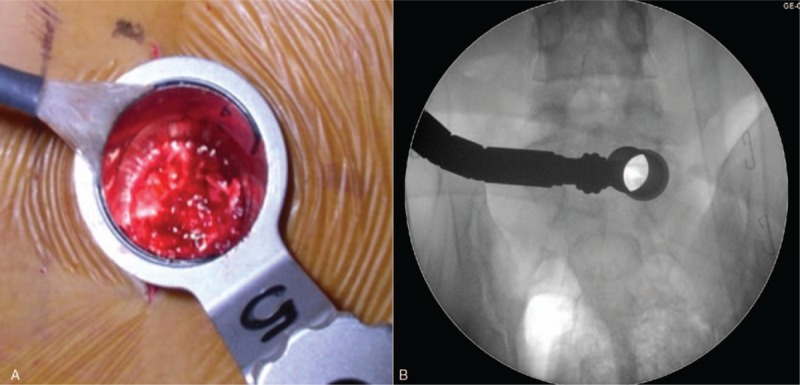
Lumbar decompressive surgery is a standard surgical technique for lumbar spinal stenosis. Many new surgical techniques have been introduced, ranging from open surgery to minimally invasive procedures. Minimally invasive surgical techniques are preferred because patients experience less postoperative pain and shorter hospital stays. However, the success rate of minimally invasive techniques have been controversial. The object of this study was to assess the feasibility of spinal decompression using biportal technique/endoscopic surgery compared with microscopic surgery.
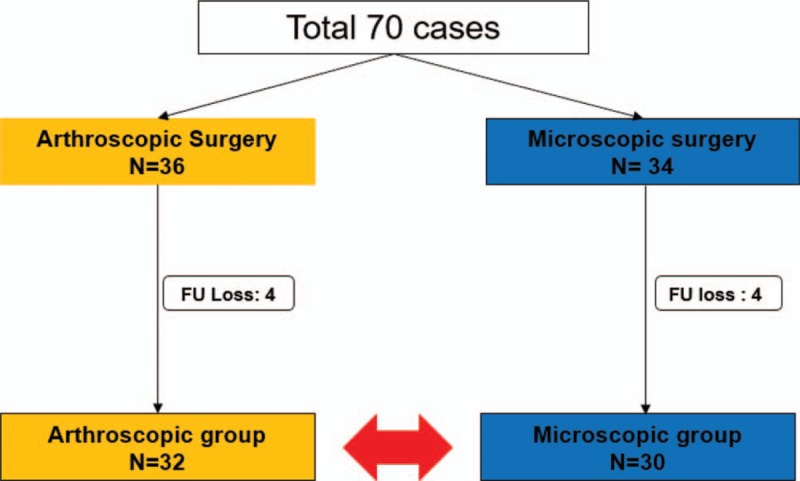
Seventy lumbar spinal stenosis patients undergoing laminectomy were included in this study. A number table was used to randomize the patients into two groups: a biportal technique/endoscopic surgery group (BG-36) and a microscopic surgery group (OG-34). One surgeon performed either biportal technique/endoscopic decompression or microscopic decompression using a tubular retractor, depending on the group to which the patient was randomized. Perioperative data and clinical outcomes at postoperative 6 months were collected and analyzed.
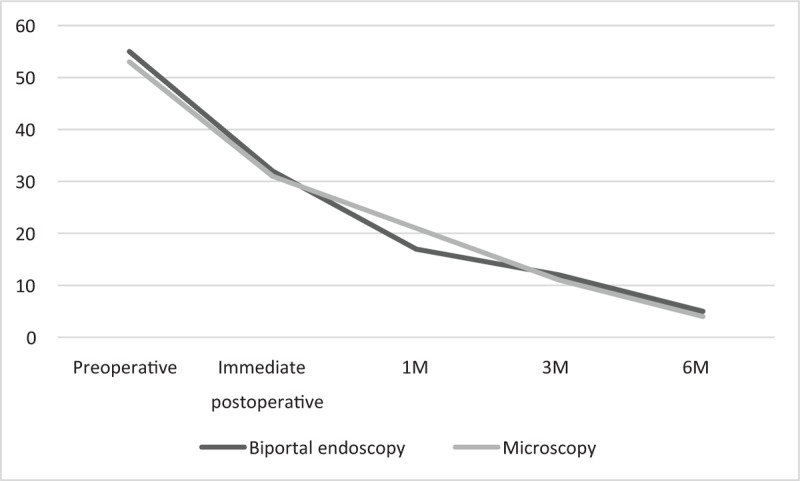
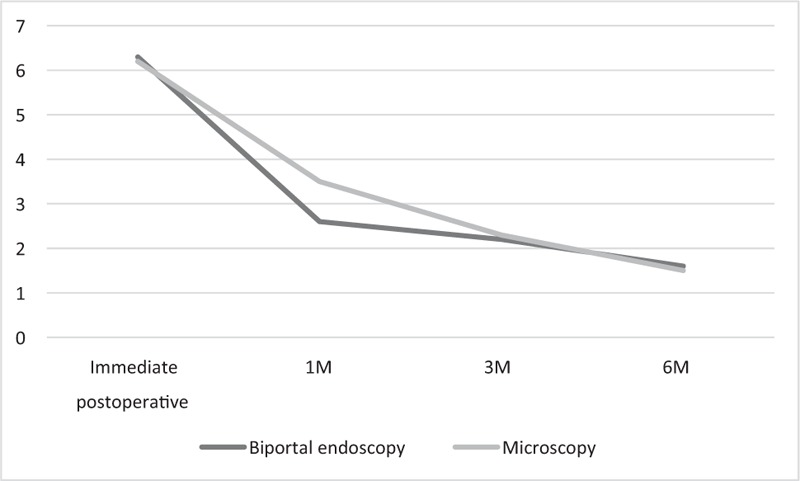
The demographic data and level of surgery were comparable between the two groups. A shorter operation time (36 ± 11 vs 54 ± 9 min), less hemovac drain output (25.5 ± 15.8 vs 53.2 ± 32.1 ml), less opioid usage (2.3 ± 0.6 vs 6.5 ± 2.5 T) and shorter hospital stay (1.2 ± 0.3 vs 3.5 ± 0.8 days) were shown in BG. The BG experienced no significant differences in clinical outcomes compared with OG. Favorable clinical outcomes were shown at 6 months after surgery in both groups.
Lumbar decompressive surgery using biportal technique/endoscopy showed favorable clinical outcomes, less pain and a shorter hospital stay compared to microscopic surgery in patients with lumbar spinal stenosis.
腰椎减压手术是治疗腰椎管狭窄症的标准手术技术。已经引入了许多新的手术技术,从开放手术到微创手术。微创手术技术更受青睐,因为患者术后疼痛较轻且住院时间较短。然而,微创手术技术的成功率一直存在争议。本研究的目的是评估双孔技术/内镜手术与显微手术相比用于脊柱减压的可行性。
本研究纳入了70例行椎板切除术的腰椎管狭窄症患者。使用数字表将患者随机分为两组:双孔技术/内镜手术组(BG - 36)和显微手术组(OG - 34)。根据患者随机分组情况,由一名外科医生使用管状牵开器进行双孔技术/内镜减压或显微减压。收集并分析围手术期数据和术后6个月的临床结果。
两组的人口统计学数据和手术节段具有可比性。BG组手术时间较短(36±11 vs 54±9分钟)、引流管引流量较少(25.5±15.8 vs 53.2±32.1毫升)、阿片类药物使用量较少(2.3±0.6 vs 6.5±2.5 T)且住院时间较短(1.2±0.3 vs 3.5±0.8天)。与OG组相比,BG组的临床结果无显著差异。两组术后6个月均显示出良好的临床结果。
对于腰椎管狭窄症患者,与显微手术相比,采用双孔技术/内镜进行腰椎减压手术显示出良好的临床效果、疼痛减轻且住院时间缩短。