Lodenstein Elsbet, Molenaar Joyce M, Ingemann Christine, Botha Kondwani, Mkandawire Jenipher Jere, Liem Loan, Broerse Jacqueline E W, Dieleman Marjolein
Athena Institute for Research on Innovation and Communication in Health and Life Sciences, VU University and KIT Gender, De Boelelaan 1085, 1081 HV, Amsterdam, The Netherlands.
Athena Institute for Research on Innovation and Communication in Health and Life Sciences Communication (VU University), De Boelelaan 1085, 1081 HV, Amsterdam, The Netherlands.
BMC Health Serv Res. 2019 May 2;19(1):279. doi: 10.1186/s12913-019-4069-2.
In Malawi, as in many low-and middle-income countries, health facility committees (HFCs) are involved in the governance of health services. Little is known about the approaches they use and the challenges they face. This study explores how HFCs monitor the quality of health services and how they demand accountability of health workers for their performance.
Documentary analysis and key informant interviews (7) were complemented by interviews with purposefully selected HFC members (22) and health workers (40) regarding their experiences with HFCs. Data analysis was guided by a coding scheme informed by social accountability concepts complemented by inductive analysis to identify participants' perceptions and meanings of processes of social accountability facilitated by HFCs.
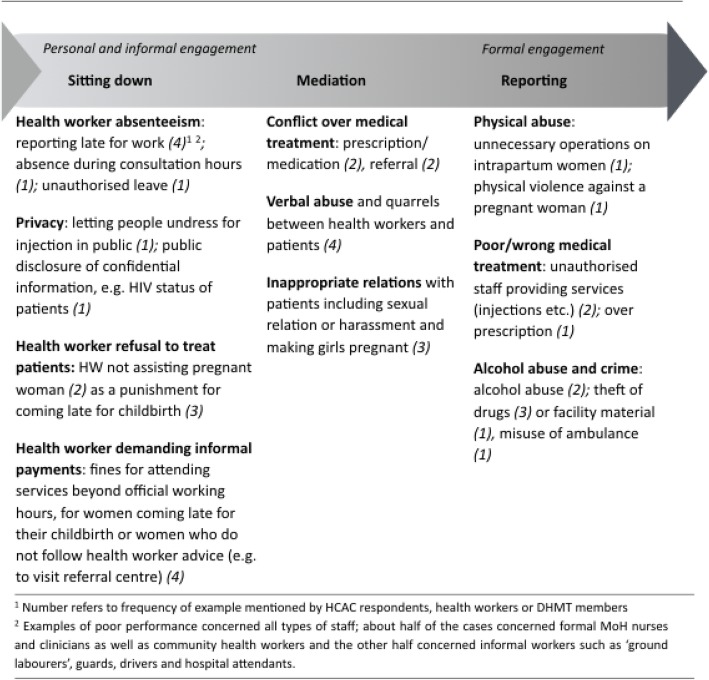
The results suggest that HFCs address poor health worker performance (such as absenteeism, poor treatments and informal payments), and report severe misconduct to health authorities. The informal and constructive approach that most HFCs use is shaped by formal definitions and common expectations of the role of HFCs in service delivery as well as resource constraints. The primary function of social accountability through HFCs appears to be co-production: the management of social relations around the health facility and the promotion of a minimum level of access and quality of services.
Policymakers and HFC support programs should take into account the broad task description of HFCs and integrate social accountability approaches in existing quality of care programs. The study also underscores the need to clarify accountability arrangements and linkages with upward accountability approaches in the system.
与许多低收入和中等收入国家一样,在马拉维,卫生设施委员会(HFCs)参与卫生服务的治理。对于它们所采用的方法以及面临的挑战,人们了解甚少。本研究探讨了卫生设施委员会如何监测卫生服务质量,以及它们如何要求卫生工作者对其绩效负责。
通过文献分析和关键信息人访谈(7次),并辅以对有目的地挑选出的卫生设施委员会成员(22名)和卫生工作者(40名)进行访谈,了解他们与卫生设施委员会打交道的经历。数据分析以一个编码方案为指导,该方案受社会问责概念的启发,并辅以归纳分析,以确定参与者对由卫生设施委员会推动的社会问责过程的看法和理解。
结果表明,卫生设施委员会处理卫生工作者的不良表现(如旷工、治疗不当和收受非正式费用),并向卫生当局报告严重的不当行为。大多数卫生设施委员会采用的非正式和建设性方法,是由对其在服务提供中的作用的正式定义和共同期望以及资源限制所塑造的。通过卫生设施委员会进行社会问责的主要功能似乎是共同生产:管理卫生设施周围的社会关系,并促进最低水平的服务可及性和服务质量。
政策制定者和卫生设施委员会支持项目应考虑到卫生设施委员会的广泛任务描述,并将社会问责方法纳入现有的医疗质量项目中。该研究还强调需要明确问责安排以及与系统中向上问责方法的联系。