1 Kinesiology and Health Science, Faculty of Health, Muscle Health Research Centre, York University, Toronto, Canada.
2 Department of Biomedical Engineering, Illinois Institute of Technology, Chicago, Illinois.
Diabetes Technol Ther. 2019 Jun;21(6):313-321. doi: 10.1089/dia.2018.0364. Epub 2019 May 6.
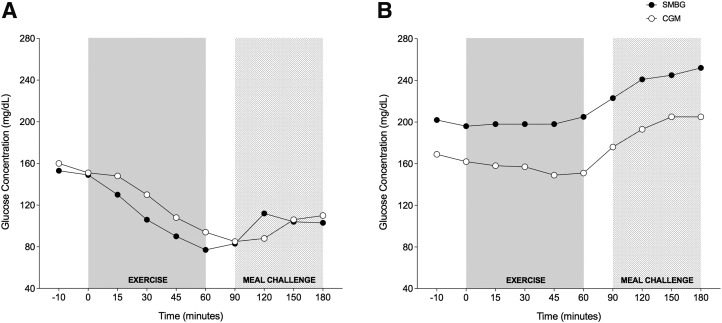
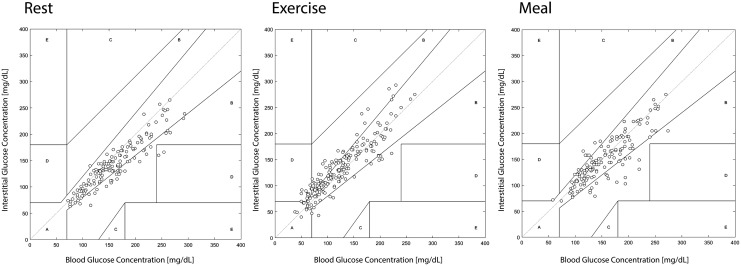
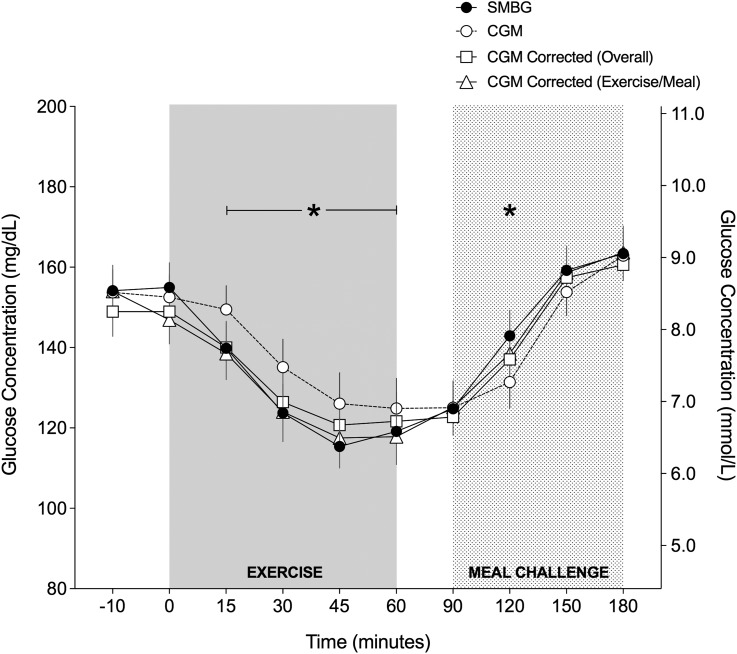
Real-time continuous glucose monitoring (CGM) devices help detect glycemic excursions associated with exercise, meals, and insulin dosing in patients with type 1 diabetes (T1D). However, the delay between interstitial and blood glucose may result in CGM underestimating the true change in glycemia during activity. The purpose of this study was to examine CGM discrepancies during exercise and the meal postexercise versus self-monitoring of blood glucose (SMBG). Seventeen adults with T1D using insulin pump therapy and CGM completed 60 min of aerobic exercise on three occasions. A standardized meal was given 30 min postexercise. SMBG was measured during exercise and in recovery using OmniPod Personal Diabetes Manager (PDM; Insulet, Billerica, MA) with built-in glucose meter (FreeStyle; Abbott Laboratories, Abbott Park, IL), while CGM was measured with Dexcom G4 with 505 algorithm ( = 4) or G5 ( = 13), which were calibrated with subjects' own PDM. SMBG showed a large drop in glycemia during exercise, while CGM showed a lag of 12 ± 11 (mean ± standard deviation) minutes and bias of -7 ± 19 mg/dL/min during activity. Mean absolute relative difference (MARD) for CGM versus SMBG was 13 (6-22)% [median (interquartile range)] during exercise and 8 (5-14)% during mealtime. Clarke error grids showed CGM values were in zones A and B 94%-99% of the time for SMBG. In summary, the drop in CGM lags behind the drop in blood glucose during prolonged aerobic exercise by 12 ± 11 min, and MARD increases to 13 (6-22)% during exercise as well. Therefore, if hypoglycemia is suspected during exercise, individuals should confirm glucose levels with a capillary glucose measurement.
实时连续血糖监测 (CGM) 设备有助于检测 1 型糖尿病 (T1D) 患者运动、进餐和胰岛素剂量相关的血糖波动。然而,间质血糖与血糖之间的延迟可能导致 CGM 低估活动期间血糖的真实变化。本研究旨在检查运动期间和运动后进餐时与自我监测血糖 (SMBG) 的 CGM 差异。17 名使用胰岛素泵治疗和 CGM 的 T1D 成年人在三种情况下完成了 60 分钟的有氧运动。运动后 30 分钟给予标准餐。使用内置血糖仪的 OmniPod 个人糖尿病管理器 (PDM; Insulet, Billerica, MA) 在运动中和恢复期间进行 SMBG 测量,血糖仪使用 Dexcom G4 带 505 算法( = 4)或 G5( = 13),这些血糖仪用受试者自己的 PDM 进行校准。SMBG 在运动期间显示血糖大幅下降,而 CGM 在活动期间显示 12 ± 11(平均值 ± 标准差)分钟的滞后和 -7 ± 19 mg/dL/min 的偏差。CGM 与 SMBG 的平均绝对相对差异 (MARD) 在运动期间为 13(6-22)%[中位数(四分位距)],进餐期间为 8(5-14)%。Clarke 误差网格显示,在 SMBG 时,CGM 值 94%-99%的时间处于 A 和 B 区。总之,在长时间有氧运动期间,CGM 滞后于血糖下降 12 ± 11 分钟,MARD 增加到 13(6-22)%。因此,如果怀疑运动期间发生低血糖,个体应通过毛细血管血糖测量来确认血糖水平。